By Tamara Straus
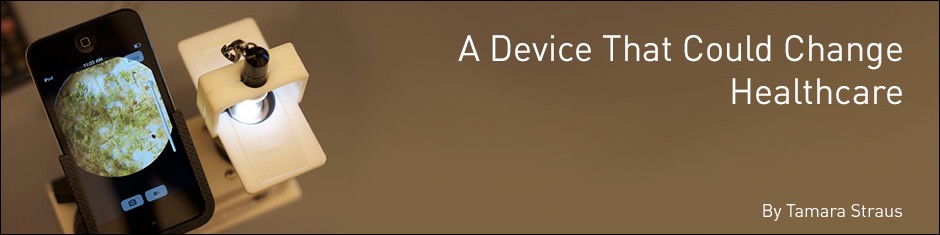
 There are three innovations without which, CellScope—a breakthrough microscopy project of Dan Fletcher’s bioengineering lab at UC Berkeley—would not be possible. They are also part of landscape of innovations that may revolutionize global healthcare.
There are three innovations without which, CellScope—a breakthrough microscopy project of Dan Fletcher’s bioengineering lab at UC Berkeley—would not be possible. They are also part of landscape of innovations that may revolutionize global healthcare.
The first is the 3D printer. Before these printers were mainstreamed, students in Professor Fletcher’s lab assembled prototype mobile microscopes from sheets of plastic that had to be cut and glued by hand. New engineering designs usually took weeks and were difficult to modify quickly. With the lab’s Stratasys 3D printer, polished prototypes are now being created in as little as a day.
The second innovation that seeded Fletcher’s leap forward in microscopy is energy-efficient LED lights. Whereas traditional microscopes rely on powerful arc lamps that cost $200 per bulb and burn less than 300 hours, the CellScope uses long-lasting LEDs that cost as little as $2.50 per bulb, provide up to 20,000 hours of use, and function on battery power in areas with unreliable electricity.
The third and probably most important innovation on which CellScope depends is the mobile phone. CellScope has been able to piggyback on tens of billions of dollars of R&D investment by cell phone companies, which have resulted in, among other things, powerful built-in cameras and the mass production of affordable components. As Fletcher pointed out in a Sept 20, 2013 Wall Street Journal op-ed:
“New phones with larger screens and better cameras may not markedly improve our lives, but the push for more powerful devices—and manufacturers’ willingness to respond to demand—is on track to improve the lives of millions of people living in extreme poverty. That’s because customers set on having the latest, greatest smartphones are driving a dramatic decrease in cost and increase in functionality that will benefit people whose total annual income is often less than the cost of a single phone.”
Back in 2006, when one-megapixel cameras started appearing on phones, Fletcher challenged students in his Optics and Microscopy class to see if the camera of a cell phone could be modified to capture images of human cells similar to those captured on his lab’s $150,000 research microscope. Continuing the project the summer after the class ended, Fletcher and a group of students attached a standard set of lenses to his sister’s Nokia phone and were able to image blood cells, malaria parasites, and the bacteria that causes tuberculosis. It was one of those moments that scientists dream of.
“We had discussions, during the course, with doctors about how broadly microscopy is used in clinical medicine, particularly in the developing world. I hadn’t realized that basic optical imaging is still so important to disease diagnosis and that the most definitive diagnosis for many diseases is seeing the actual disease-causing agent in a patient sample,” said Fletcher. “That’s when I realized that if we could do microscopy properly on a mobile phone, the device could be very useful.”
Not only was the potential for disease diagnosis outside of hospital infrastructure considerable, Fletcher and his team knew that mobile manufacturers were in a race to integrate phone cameras with computation, SMS, email, Internet access, and friendly user interfaces. In a few short years, this would mean that CellScope could provide diagnostic solutions at pretty much the same rate as any digitally enhanced microscope in a well-equipped hospital.
 Members of the Fletcher lab could even foresee a time when patients’ blood or sputum smears could be imaged with a mobile digital microscope and then—using a computer algorithm for automated disease detection—proceed immediately to treatment, without the patient stepping foot in a city hospital or medical lab. It would mean, for example, that tuberculosis, which annually kills more than 2 million people and sickens approximately 15 million, could be tackled in places where laboratory facilities are scarce but mobile phone infrastructure is extensive. It would mean that a new point-of-care diagnostic was possible for many diseases that go undiagnosed in many countries, ranging from debilitating eye disorders to chronic blood parasites.
Members of the Fletcher lab could even foresee a time when patients’ blood or sputum smears could be imaged with a mobile digital microscope and then—using a computer algorithm for automated disease detection—proceed immediately to treatment, without the patient stepping foot in a city hospital or medical lab. It would mean, for example, that tuberculosis, which annually kills more than 2 million people and sickens approximately 15 million, could be tackled in places where laboratory facilities are scarce but mobile phone infrastructure is extensive. It would mean that a new point-of-care diagnostic was possible for many diseases that go undiagnosed in many countries, ranging from debilitating eye disorders to chronic blood parasites.
The Fletcher Lab began making its case for the potential impact of CellScope slowly, as it was a side project in a lab focused on making cutting-edge biophysical measurements of cells. In May 2007, CellScope won a Big Ideas@Berkeley award of $8,500, and in January 2008 it received a $100,000 grant from Microsoft Research. By May, The Economist, ABC, Wired, and other media had picked up news of CellScope. In April 2009, the team won another $100,000 grant from Intel’s Inspire-Empower Competition, followed by support from the Vodafone Americas Foundation. And in July 2009, it published its first academic journal paper—in PLoS ONE, documenting how CellScope captured images of the parasite that causes malaria in humans, the bacteria that causes tuberculosis, and sickle-shaped red blood cells. The team also showed in a 2012 National Institutes of Health paper how their images of tuberculosis bacteria could be automatically counted using image recognition software.
By 2011, CellScope had raised a total of $500,000, thanks to additional grants from the Bill & Melinda Gates Foundation, UC Berkeley’s Blum Center for Developing Economies and the Center for Information Technology Research as well as the Vodafone Americas Foundation, and was ready to field test its first device.
Its first large field experiments took place at health clinics in Hanoi Province, Vietnam. In partnership with the Vietnam National Tuberculosis Program and the University of California, San Francisco, Fletcher’s group deployed 15 CellScopes for a full year, to evaluate their uptake and ability to detect TB at health care facilities with little medical or IT infrastructure. The Hanoi Province pilots showed that community health care workers were able to operate the CellScope and that disease diagnosis met the standard quality available at major Vietnamese hospitals. This work motivated development of a second generation device that is being tested in Hanoi.
Recently, another CellScope device was field-tested in Cameroon where the Gates Foundation and the U.S. National Institutes of Health had been struggling to find a way to restart mass drug administration programs to fight the roundworms that cause river blindness and lymphatic filariasis. The problem health workers faced was that patients were at risk of serious health complications, including death, if they were given river blindness medication while co-infected with the Loa loa worm. But to test for Loa loa, health workers needed to draw several milliliters of blood and prepare two blood smears for observation under a traditional microscope—costly and time-consuming steps impossible to carry out across the country. Health programs were basically stuck; they could not proceed with large-scale treatment.
Then in February 2014, CellScope trials of 120 people proved adept at counting Loa loa worms, using only a finger prick of blood and a few minutes of analysis time. The trials also validated CellScope’s automated detection of worms in whole blood, and thus the elimination of time-consuming lab diagnosis. Larger tests involving thousands of patients are planned for 2015.
“The Loa loa trials may be the ones that allow us to bring the CellScope to scale in developing regions,” said Clay Reber, a UC Berkeley master’s student in bioengineering who has been on the CellScope project since 2010. “They could show that the CellScope meets conventional diagnostic methods and will be cheaper and easier to use than current methods. They could enable the much-needed mass drug administration programs against river blindness to restart. Worldwide, there are 130 million people at risk of being infected with the river blindness worms and about 13 million people with Loa loa.”
Another testing ground for CellScope devices is Thailand, where there are only 648 ophthalmologists for the entire country (1.52 doctors per 100,000), with most located in the urban centers of Bangkok and Chiang Mai. Cytomegalovirus (CMV) retinitis, which disproportionally affects HIV patients and can lead to blindness, is treatable, but infection rates are high and diagnosis rates are low. Since 2012, community health workers and other non-specialists have a half dozen Ocular CellScopes to test their utility for patients at risk of CMS. Results are forthcoming.
Professor Fletcher admits it’s challenging to address the many diagnostic opportunities that CellScope could address simultaneously. “The key,” he said, “is great collaborators—great clinical collaborators who have embraced the technology, contributed to its design and implementation, and allowed us to plug into existing field studies and test sites with this alternate technology.”
 With so many potential applications and field tests for CellScope, it is no wonder that the team has at times felt overstretched. CellScopes have been sent and used literally around the world. In Hawaii, the education nonprofit Kahi Kai is using the mobile microscopes to collect data for various water quality indicators, such as plankton. In Egypt, Dr. Annika Guse of Heidelberg University took CellScope for coral reef monitoring. There is even a CellScope in Antarctica, and Parisian artist Geneviève Anhoury is opening a show this December using images taken with a CellScope.
With so many potential applications and field tests for CellScope, it is no wonder that the team has at times felt overstretched. CellScopes have been sent and used literally around the world. In Hawaii, the education nonprofit Kahi Kai is using the mobile microscopes to collect data for various water quality indicators, such as plankton. In Egypt, Dr. Annika Guse of Heidelberg University took CellScope for coral reef monitoring. There is even a CellScope in Antarctica, and Parisian artist Geneviève Anhoury is opening a show this December using images taken with a CellScope.
Perhaps the strongest example of CellScope’s wide applicability and embrace is its for-profit spinout, CellScope, Inc. In June 2013, Khosla Ventures invested $1 million in the company founded in 2010 by Erik Douglas and Amy Sheng, two former students of Professor Fletcher’s. Since then, the company has secured additional funding on the promise it will create a “smartphone-enabled digital first aid kit.” CellScope Inc.’s first product is an iPhone otoscope that enables parents and physicians to remotely diagnose ear infections in children, an ailment that results in an estimated 20 million U.S. doctors visit per year. The release date for the otoscope is set for 2015. Douglas said 800 doctors and clinicians have been testing it since last December, and 100 California families have been using the device at home.
For Fletcher, the CellScope represents not so much new science as a new approach to the old problem of disease diagnosis, one that moves clinical microscopy forward by solving integration, implementation, and usability challenges. “I think it’s really exciting to see how a technology that has come from an academic lab, was created on a 3D printer, and is intended for use by minimally skilled healthcare workers can help someone in a developing region receive better healthcare and maybe even help seed an industry here in the U.S,” he said. Fletcher has no objections to the domestically oriented for-profit spinout, but hopes “there is continued attention—and funding—to support solving the often very different healthcare problems of developing countries with these devices.”
Fletcher’s mind tends toward scientific skepticism, toward the need for real-world proofs and repeatable results. But he is willing, after some urging, to forecast his device’s possible impact. “My hope is that CellScope will present a new way of delivering healthcare,” he said. “It has the potential to provide much faster access to disease diagnostic information as well as more regular information about our own healthcare. Our technology is part of a fundamental change in healthcare that will see each of us able to take much better care of ourselves by collecting and analyzing personal health data with devices like mobile phones. And CellScope is just one device in that direction. The mobile healthcare revolution has begun.”


