A new member of the Graduate Group in Development Engineering, Ceferino and his team move in after disasters, working on the ground to understand how and why infrastructure fails — and how governments can build city systems that are better equipped to withstand the next one.
A series of devastating earthquakes struck Turkey and Syria in 2023, killing more than 55,000 people in one of the region’s deadliest natural disasters in decades.
In the aftermath, search and rescue teams struggled to operate after their own equipment was damaged. Hospitals collapsed, forcing injured survivors to travel long distances to access urgent medical care.
Prof. Luis Ceferino
According to Luis Ceferino, an expert in disaster risk and modeling, multiple emergency response systems failed at once — including communications, rescue operations, and power infrastructure — disrupting what engineers call the “earthquake survival chain.”
But for Ceferino, this is where the work begins.
An assistant professor of Civil and Environmental Engineering at UC Berkeley, Ceferino and his team move in after disasters, working on the ground to understand how and why infrastructure fails — and how governments can build city systems that are better equipped to withstand the next one.
He’s conducted post disaster field research all across the world. His work, including collaborations with institutions like the World Bank, examines risks to housing, hospitals, schools, and energy infrastructure in countries like the United States, Nepal, Pakistan, Uzbekistan, the Kyrgyz Republic, and Peru.
“(My work) gave me a lot of experience to start thinking about these questions, about failures of infrastructure and how they impact access to services that are very important after a disaster,” he said.
“What I’m hoping to do with my work is inform governments of the best ways to invest in making things more resilient.”
Now, Ceferino is bringing that experience to the classroom as one of the newest faculty members to join UC Berkeley’s Graduate Group in Development Engineering. As a new addition, he invites MDevEng students to participate in his research, mentoring them as they develop their own capstone projects. He also encourages students to take his recurring class, Disaster Risk Analysis: a course that introduces students to modeling extreme events and assessing which infrastructure systems are most vulnerable.
His interest in disasters began in Peru, where he grew up along the seismically active Ring of Fire, a belt of frequent earthquakes and volcanic activity encircling the Pacific Ocean. As a civil engineering student at the Universidad Nacional de Ingeniería in Lima, he witnessed firsthand how infrastructure failures can cut off access to essential services.
That early exposure shaped his focus on disaster prevention, particularly for communities with fewer resources at their disposal.
“In civil engineering, we want to create better technology to improve the resiliency of society to these extreme events. One approach is to make things stronger — but that’s expensive,” he said. “I was very interested in the regional scale: ‘What can you do to make an entire city better if you have limited resources?’”
Over the course of his career, Ceferino has studied disasters ranging from earthquakes in Latin America to hurricanes in the United States.
He noted, however, that fieldwork often changes the way he thinks about how engineers model risk, how communities respond, and how unexpected factors can influence recovery.
After Hurricane Sandy in 2012, he visited flooded neighborhoods in New York and New Jersey. In some coastal communities, flooding caused by the storm meant a sharp drop in home values, and homeowners still had mortgages to pay.
Many residents couldn’t afford to rebuild, and the local real estate market meant that houses couldn’t be sold and families couldn’t relocate,causing conditions in these disadvantaged areas to worsen drastically.
In the following years, the market became depressed. Traditional disaster risk models — which estimate repair costs and timelines based on materials, labor, and available funding — could not fully capture what many impacted families were experiencing.
For Ceferino, the experience highlighted the importance of considering factors outside of engineering, such as economic and market dynamics, into disaster risk analysis — serious impacts of extreme events that go beyond physical destruction.
“There are many instances in which we’re on the field and we talk to people, we see the infrastructure, and we learn new things about the mechanisms that control decision making in recovery experiences and disaster response,” he said. “Oftentimes it’s just different from how we thought.”
Experiences like these have also reinforced for Ceferino the importance of interdisciplinary approaches to disaster response. Engineers alone cannot solve these problems, he argues; economists, policymakers, and educators all play a role in shaping recovery.
Additionally, Ceferino believes that bringing in diverse perspectives can help engineers improve risk models, and also inform policies that guide recovery and prevention.
“If you’re repairing schools, you need someone who will prepare a plan for moving students around to ensure the learning objectives are not lost while you’re repairing infrastructure,” Ceferino said.
That perspective is what drew him to Development Engineering, a program that brings together students in disciplines ranging from global health to AI and data analytics to address the world’s most pressing humanitarian issues.
The MDevEng is a 15-month program that prepares students for careers in social impact. Students take on a number of hands-on projects, including a summer internship and a final capstone project.
In his Disaster Risk Analysis course, MDevEng and other students will learn the fundamentals of modeling disasters and predicting how infrastructure systems respond to extreme events. The class culminates in an open-ended project, where students apply their studies to real-world scenarios.
Last semester, Ceferino advised some MDevEng students with projects spanning risk modeling and disaster impacts — from analyzing how home elevation affects flood exposure in New York to using satellite imagery to track power outages after the Los Angeles wildfires.
In joining the DevEng Graduate Group, he formally supports MDevEng students with capstone projects, where some will have hands-on opportunities to work with Ceferino’s research group. This coming Fall, students working with Ceferino on their MDevEng capstone will be involved in projects such as modeling non-recovery pathways in coastal communities facing flood risks, as well as studying hospital earthquake response strategies via immersive virtual reality. He said he is currently focused on integrating into the program’s community and getting to know students, but hopes to eventually expand collaboration by co-advising capstone projects with other faculty.
Beyond the data and modeling, Ceferino sees his DevEng affiliation as an opportunity to join a vibrant, collaborative community.
“I think students just take an idea and give it its own direction, which is amazing,” Ceferino said. “I’m excited to be part of that kind of community and learn more about the students who come through the program.”
Casillas Rios, a three-year student fellow at the Blum Center, graduated this May from the Global Poverty & Practice minor. Since high school, she’s been committed to enhancing the quality and availability of public green spaces in her community.
Growing up in Los Angeles’ San Fernando Valley without a backyard, Yesenia Casillas Rios would turn to local parks as a way to get outside, play, and explore her neighborhood.
These communal open spaces “were very crucial to the way I grew up,” she says.
In her senior year of high school, Casillas Rios became more directly involved in her local public spaces when she started doing a volunteer youth program at Black Thumb Farm, a community farm a couple blocks from home. Her end-of-the-year project tracked the impacts of weather on plant growth.
“They taught me a lot about food justice, food sovereignty, and environmental justice in terms of where we lived and how our environment had a lot to do with how we experience our day-to-day lives as low-income, first-generation students,” she said.
The experience set her down a path to UC Berkeley, where the landscape architecture major graduated this month from the Global Poverty & Practice minor, or GPP, which allowed her to stay involved with Black Thumb Farm during college. For the past three years, Casillas Rios has also served as a Fellow at the Blum Center, where she has provided essential administrative and event support for the Master of Development Engineering program.
While looking at colleges in high school, Casillas Rios discovered a Berkeley program that spoke directly to her experiences and interests.
“I found out about landscape architecture and how, as a landscape architect, you could design parks or you can design green spaces,” she said. “That fascinated me.”
It’s an interdisciplinary field, and, once on campus, Casillas Rios looked for other opportunities to interact with people from different disciplines. Landscape architects “care about energy, they care about water, they care about communities,” she said. The Blum Center, she found, fit that description, too.
In her student associate role, she worked closely with then–Assistant Director of Student Affairs Valerie Moss, who introduced her to GPP. The minor had clear parallels with Casillas Rios’ passion for community development.
A lesson in soil and plant health at Black Thumb Farm (Photo by Yesenia Casillas Rios)
“I’ve always liked to learn as much as I can,” she said, “and GPP also has to do with students from all sorts of different interests and backgrounds who are also interested in change, are hopeful for change, and want to learn how we can create that change.”
Her first GPP class, “Global Poverty: Challenges and Hopes,” doubled as one of her major requirements. “‘I’ll give it a shot,’” she remembers thinking. “And I fell in love with the class.” Prof. Sai Balakrishnan’s passion for understanding global poverty inspired her to officially pursue the minor.
Casillas Rios returned to Black Thumb Farm during school breaks to do her practice experience. And this time, she led the high schoolers.
The farm had a community-supported agriculture (CSA) model, and Casillas Rios led these youth in growing a variety of vegetables they would then sell to locals participating in the CSA. On weekends, she taught them what kind of flowers could grow in what conditions and how to arrange the flowers for selling. She also led workshops that the farm put on.
The farm also asked their resident landscape architect to help design a new plot of land they had, two blocks from Casillas Rios’ childhood home. This included interpretive landscape maps to engage the city on the farm’s expansion plans.
The full-circle nature of her journey isn’t lost on her.
“It’s such a beautiful thing,” she said, “I first came in just wanting to have a green space in my community, and now they’re bringing so much back to us — providing so many community workshops, community engagement.”
Earlier this month, Casillas Rios finished up her three years supporting the Blum Center’s programs and activities, and on May 19, she and 32 others from 18 different majors graduated from the GPP Minor.
She credited Moss and one of her GPP professors, Clare Talwalker, with encouraging her to reflect more on her interests, what she chose to do during college and why, and to be more open-minded about what she could pursue academically and professionally.
“It was a pleasure having Yesenia in class!” Talwalker said. “She brought to discussions her investment in understanding how our access and uses of built spaces, including green spaces, intersect with poverty and inequality, and how the design and shaping of landscapes might be socially transformative.
“Her contributions were unique, valuable, and inspiring.”
Over the years, Moss and Chetan Chowdhry, the Center’s Director of Student Programs, had also helped build a feeling of community at the Center by approaching Casillas Rios as more than just a student worker.
“I’ve become so close to them after these three years. It helped me a lot in not feeling so alone in this journey as a first-generation student and going to college,” she said. “I’m not just doing it to do it, like many of us are, but I’m here to do it for a purpose. Feeling reminded of that purpose with those reflections that I was able to have with them was something I’m truly grateful for.”
This summer, Casillas Rios will finish up an internship at a landscape architecture firm and another energy-focused internship at a consulting group. Her plans beyond that aren’t settled, but she knows she wants to eventually attend graduate school and gain more hands-on experiences in and around the landscape architecture space.
She will also be heading back home soon to the San Fernando Valley, and to Black Thumb Farm.
“Every time I’ve gone back on breaks,” she said, “they’re like, ‘You’re going to come back once you graduate; you’re going to take charge of this.’”
Would she?
“Imagine,” she said with a laugh. “You never know. I really don’t know where I’m going to be. But I’ll for sure still be helping them out as well.”
Through roles with the International Rescue Committee, UNICEF, UNFPA, and Columbia University School of Public Health, Navani spent years building health data systems in conflict and disaster settings. She describes a pattern that kept surfacing across the more than 15 countries she’s worked in: The groups facing the steepest health risks were also the ones least visible in the data systems.
In regions upended by conflict and climate threats, how do you devise health systems and strategies for groups that don’t access formal health systems or show up in existing data?
It’s a challenge that Sonia Navani, an implementation scientist and Blum Senior Fellow, has been working on for decades with refugee and displaced populations.
Through roles with the International Rescue Committee, UNICEF, UNFPA, and Columbia University School of Public Health, Navani spent years building health data systems in conflict and disaster settings. She describes a pattern that kept surfacing across the more than 15 countries she’s worked in: The groups facing the steepest health risks were also the ones least visible in the data systems.
That invisibility wasn’t random. It largely tracked with what she calls “more granular gradients of poverty — who could reach a clinic early, who showed up late, and who never showed up at all.” As digital health and AI-enabled tools started showing up in some of these settings, Navani says many of them inherited those same blind spots.
But what shifted her thinking wasn’t just who was missing from the data. It was what she was seeing climate change do. In the communities she works in, floods and extreme heat aren’t just making food harder to get — they’re changing what people eat, when they can get it, and how often those disruptions hit.
Navani describes this as going beyond the familiar picture of food insecurity. It’s actively reshaping dietary patterns in communities already stuck in poverty, and driving chronic disease risks that didn’t exist in the same form a generation ago. The health tools being extended to these settings, she says, were designed for more stable situations where diets and environments don’t shift seasonally.
What struck her wasn’t just that the problems were getting worse. It’s that these disruptions are forcing changes in how communities live, eat, and cope — and those changes are visible and trackable, and in some cases connected to things that are low-cost and doable without relying heavily on outside aid.
Navani’s current work focuses on one area where she’s building this out — food-based nutrition for women in early pregnancy — but she says the problem is much bigger than nutrition.
“Communities in poverty are generating observable signals, particularly related to long-term chronic disease risks such as diabetes and asthma, but most existing tools are a mismatch — preconditioned on stability,” she said. “The signals don’t translate into contexts that are anything but stable, and where different aspects of that poverty contribute to whether disease risks compound or not.”
Her response has been to try to build something that goes beyond fixing data shortages. She wants to connect what’s coming out of climate science and biology so that the tools are looking for earlier signs of disease risk — but designed for unstable conditions instead of stable ones. She says this is getting more urgent in communities where health systems aren’t set up for chronic disease prevention, let alone treatment.
A framework she has developed for this purpose she calls Precision Community Health. She describes it as “a translational approach that applies representational learning to identify when deprivation shapes disease risk at a community scale — providing pattern-level profiles for chronic disease mitigation where epigenetic mechanisms are a major influence on disease risk — alongside individual genetic risks.”
So what does that actually look like on the ground? For Navani, putting this into practice meant building a whole process — not just the AI part, but how you get useful evidence out of communities that formal research doesn’t reach, how you connect that to science that works under unstable conditions, and how the results get back to health workers in a form they can actually use.
She founded DHDI, a nonprofit research group, to explore these areas with local civil society partners, from generating data ethically with communities, to figuring out where the real traction points are for preventing disease under climate stress and poverty, to getting support back to women and health workers in ways they can act on.
For Navani and her team, the community comes before any data generation or code. They developed Climate Health Photovox, a 26-session curriculum running with local partners in eastern DR Congo. It’s a digital storytelling program where women learn not just how but why climate events are reshaping local agriculture and food, and what that means for family health.
Using shared smartphones, women document those shifts themselves: photographing local foods, tagging them with local names and seasonal details. Navani describes it as building a visual record of what’s happening through the eyes of the very groups that existing systems tend to miss.
She notes that women who may not own phones but regularly use them within households become participants in shaping both the questions and the evidence — “not as data subjects, but as co-investigators,” as she puts it. The curriculum was designed to stand on its own. Women come away with food and nutrition strategies, smartphone skills, and connections to other communities dealing with similar climate challenges. But the images they share also feed into the AI work, and Navani says that dual purpose is built in from the start.
Of the different health problems where this kind of community-generated data could be put to use, Navani started with nutrition for women in preconception and early pregnancy. She calls it the area where the signals are most clear, the interventions are affordable, and there’s a specific biological window where acting early matters most.
The food images and the image meta-data feed into EpiNu, a proof-of-concept AI system that Navani says was built for the conditions where most tools fall apart — offline, low connectivity, no text input, no self-reporting. The system runs on a micronutrient database her team built specifically for preconception and pregnancy.
Navani explains that standard nutrition data often doesn’t reflect what people actually absorb from food — not just what’s in it. She gives the example of iron in beans: Guidelines list the iron content, but compounds in the food can block most of it from being absorbed.
EpiNu tries to account for that gap. The system is aimed at community health workers, giving them guidance based on what’s locally available rather than general recommendations that Navani says rarely match reality for women dealing with both poverty and climate disruptions.
The focus on early pregnancy, she says, is where the science and the urgency come together. There’s a narrow window early on where what a woman eats can have lasting effects.
“Many women don’t access clinical care until well after those early windows have closed,” Navani said. “In DR Congo, this is showing up in the data — excessive neural tube defects, a largely preventable problem where folate is a major factor. Supplements remain central, but many women receive them too late, if at all. The question is what can be done with food already in the household to unlock more of what these women need.”
The urgency behind this work isn’t abstract for Navani. Darfur remains the clearest example.
In 2004, she helped set up data systems in displacement camps in South Darfur and returned over the following years to support local teams, only to find the same women in the same makeshift shelters under the same conditions.
“They would remember me, which was both amazing and horrifying,” she recalled. “Horrifying because it meant they were still there — the same people, in the same tents made of plastic sheeting. The only thing that changed was the international actors around the table.”
That lesson has only gotten sharper. Darfur is in extreme crisis again.
“If the architectures of aid systems in place for decades have reached their limits,” she said, “then the question is not how to rebuild them in their original form for a world that doesn’t exist anymore, but how to rethink them entirely — and whether the computational tools now available might, for the first time, make that possible.”
At the Blum Center, Navani works with students in computer science, data science, computational social science, developmental engineering, and other fields. She says the projects push students to deal with constraints they don’t usually face.
“Most computational models are built in and for stable, well-resourced environments, then treated as universally applicable,” she said. “Working on EpiNu pushes students to rethink those assumptions — what counts as sufficient data, what ethical data collection looks like under conditions of partial access and shared devices, and what scalability actually means when infrastructure cannot be taken for granted.”
Looking ahead, Navani and her team are expanding their work in eastern DR Congo with larger networks of local partners. The bet, she says, is that building for the hardest conditions first actually makes scaling easier, not harder.
“If you design for eastern DRC and it works, moving into higher-infrastructure settings for communities experiencing poverty is a much shorter leap than trying to go the other direction,” she said. “Most people assume you build for stability and adapt down. We think it’s the other way around.”
She comes from a long line of tea farmers who cultivated the land long before global supply chains and corporate monopolies reshaped the region’s tea industry. Though she didn’t grow up on the farms full time, that history shaped how she understood land and labor.
Shreya Chaudhuri — an alumna of UC Berkeley’s Global Poverty and Practice (GPP) minor — was raised in the Bay Area, but she spent her summers thousands of miles away in eastern India, on her family’s tea farms in Assam.
She comes from a long line of tea farmers who cultivated the land long before global supply chains and corporate monopolies reshaped the region’s tea industry. Though she didn’t grow up on the farms full time, that history shaped how she understood land and labor.
Her mother carried that connection closer to home, spending time with Chaudhuri outdoors along the Bay Area’s beaches and among the redwood forests. Chaudhuri often tagged along while her mother gardened.
“I would mostly be talking,” Chaudhuri said, laughing. “But I was still with her outside.”
From those early experiences, Chaudhuri absorbed a philosophy that would shape her worldview and pull her towards environmental justice.
“Live in reciprocity with the land, respect the earth, and respect nature,” Chaudhuri said. “Never take more than you give.”
In middle school, Chaudhuri’s science teacher encouraged students to design their science fair projects around real-world problems, which stuck with her as she discovered her own interest in environmental science.
She found her footing during her senior year of high school, where her project on lead pollution in sub-Saharan Africa explored how algae could be used as a nature-based solution to remove heavy metals from water.
The project earned international recognition and was published with UNESCO, but more importantly, she said, it reframed her relationship to science — seeing it as a means of addressing inequality and environmental harm.
Chaudhuri doing field research in agroforestry (courtesy photo)
Her love for the environment would ultimately define her time at UC Berkeley, where she graduated in Spring 2025, received the Stronach Prize, and returned soon after to serve as a visiting scholar. Over the course of her education, Chaudhuri combined technical training in the sciences with political analysis, double majoring in environmental science and geography with an additional minor in data science.
The GPP minor program, however, is what Chaudhuri said truly “laid the foundation” for work with local communities in India.
The Global Poverty and Practice minor program, offered through the Blum Center of Developing Economies, challenges students to examine the structural roots of poverty and inequality while applying academic learning to community-engaged work.
Upon arriving at UC Berkeley, Chaudhuri planned to pursue a technical career in environmental microbiology. But after spending a summer working full time in a lab at the Carnegie Institution for Science her freshman year, she realized something was missing.
“There were already so many climate solutions,” she said. “But there wasn’t a bridge between the people who needed them the most and the people who were building them.”
Chaudhuri said that after taking several courses in the GPP minor, she was convinced the program could offer her something that no others at Berkeley could: coverage of perspectives from the Global South on climate change.
That focus shaped how Chaudhuri approached her GPP practice experience. Encouraged by GPP faculty to work with communities they were already part of, Chaudhuri centered the project on her own community in Assam. A defining element of the program, the practice experience is designed to help students bridge theoretical frameworks with real-world poverty action.
Chaudhuri with her parents and uncle at a Durga temple built by her great-grandfather on the tea farm in 1935 (courtesy photo)
She got the inspiration from a trip to India over two years ago, when she returned to her uncle’s tea farm and saw firsthand how farmers were reviving Indigenous agricultural practices — such as polyculture, mulching, and composting — in response to climate change and corporatization.
“It was incredible to see the on-the-ground work that’s happening in frontline communities,” Chaudhuri said. “I wanted to be able to go back into my community and help co-create something meaningful together.”
After learning more about her own family’s historic struggle with colonial rule over their farmland, Chaudhuri decided to document these Indigenous ecological methods while also examining colonial tea plantations in Assam and how colonialism has shaped the community’s ecology and geography.
That research expanded into her senior theses and, later, became the basis for the follow-up initiative — Equi-Tea: মাটিৰ মুক্তি, মানুহৰ মুক্তি (“liberation of the land is liberation of her people”) — that earned her the prestigious Judith Lee Stronach Baccalaureate Prize.
Through the prize, Chaudhuri is working with farmers today in Assam to build a direct-to-consumer tea brand rooted in those same Indigenous ecological principles. The model prioritizes organic cultivation and farmer-led decision-making, while cutting out corporate intermediaries that often absorb the bulk of profits. Even well-meaning brands limit farmer autonomy, she said, and don’t use the surplus profits to reinvest in the agrarian communities, who are struggling to transition to agroforestry. Chaudhuri’s brand aims to emphasize local economies, ecologies, and autonomies, while building bridges between the producers and consumers — something that the colonial supply chain sought to eradicate.
To tell their story, Chaudhuri is producing a short 30-minute film, drawing on interviews with farmers and footage from the fields. The goal, she said, is to show American audiences how tea farmers are struggling with climate change, colonial legacies, and global markets.
“They’re focused on daily survival and making sure that their tea farms last and exist; they don’t have the capacity to build out the storytelling and marketing models that a lot of brands in America do,” Chaudhuri said. “I want people to know what tea farms are going through because it is a microcosm of the climate crisis.”
She also brought this work back to UC Berkeley last summer through an interactive tea exhibition at the South and Southeast Asian Library in partnership with the Institute of South Asia Studies. While she worked as a Climate Action Fellow at the Student Environmental Resource Center, she created a campus café pop-up, where visitors could sample tea grown ethically using Indigenous methods.
Chaudhuri at a workshop on Indigenous burning traditions that she hosted with the Project Planet team at the International Science & Engineering Fair’s Education Outreach Day (courtesy photo)
Alongside her work on tea, Chaudhuri emphasized the importance of climate education, something she’s been actively pursuing since she was 16 when she founded Project Planet, a nonprofit dedicated to decolonial environmental education. On campus, this took shape as the Decolonizing Environmentalism DeCal she founded, as well as the Decolonial Environmental Network and American Cultures Environmental Justice Initiative.
Across all her experience, however, Chaudhuri stresses the importance of paying attention to how climate change is experienced on the frontlines, as well as to the Indigenous science, often overlooked in mainstream climate research, that communities already use to adapt to changing conditions.
“The majority of the people in this world are at the margins of the climate conversation, and we have to center their stories,” Chaudhuri said. “We have to center their narratives.”
“The gift of Development Engineering, to me, is learning to think about the technical and the human in the same hand,” commencement speaker Pratiyush Singh told his peers and their guests. “I leave with a way of seeing: one that showed me that who I am and what I want to do are not competing worlds, but the same story.”
The Master of Development Engineering program graduated its fourth cohort last month, expanding the ranks of professional changemakers addressing complex challenges in low-resource settings around the world
Families of the 27 newly minted graduates gathered in Banatao Auditorium for an intimate commencement ceremony before moving to Blum Hall, home of the MDevEng program, to celebrate.
Pratiyush Singh (center) with Professors Kara Nelson (left) and Amy Pickering
“The gift of Development Engineering, to me, is learning to think about the technical and the human in the same hand,” commencement speaker Pratiyush Singh told his peers and their guests. “I leave with a way of seeing: one that showed me that who I am and what I want to do are not competing worlds, but the same story.”
The Class of 2025 studied water-quality solutions for Passamaquoddy communities in Maine, conducted a lifecycle sustainability assessment of post-consumer PET recycling in Uganda, worked on AI-based portable diagnostics for neglected tropical diseases, and envisioned what a car-free San Francisco would need and look like — among many other projects, research, innovations, and efforts to apply engineering and other fields for the benefit of people and planet.
And they pursued this work while often-unprecedented challenges to higher education, research, and the very means and goals of Development Engineering were unfolding over the cohort’s three semesters at Berkeley.
“This year has been an incredibly difficult year to think about justice and development: one marked by funding cuts, institutional uncertainty, and the painful realization that the very work we’re trained to do often stands on fragile institutions,” said Singh, whose capstone project focused on shifting mortality burdens among vulnerable populations facing extreme heat in Mexico. “If anything, this fracture makes our work much more urgent, much more necessary.
“Justice is never guaranteed by institutions,” he added. “It survives because people, hopefully us, choose to carry it forward.”
Paige Balcom
Paige Balcom, who received her PhD designated emphasis in Development Engineering in 2022, returned to Berkeley for the first time since earning her degree to give the evening’s keynote address.
She shared some of the challenges that the social enterprise she co-founded, Taktaka Plastics, has faced, and how managing and motivating people — a process built on trust — is a more difficult component of DevEng work than the technical issues.
DevEng “is long-game work,” she said. “And at the center of that long game is trust.”
Trust is “built through listening, showing up consistently, and involving the stakeholders of partners, not just the beneficiaries. Trust is built through co-design, through transparency, and doing what you say you’re going to do,” said Balcom. “And trust is fragile; it can be damaged quickly: by rushing, by ignoring local knowledge, or by prioritizing short-term wins over long-term relationships.
“But when stakeholders trust you enough to give their honest feedback, and you authentically incorporate their input and design,” she said, “the solution will be much better, and it will have a much higher chance of actually being used long term.”
Balcom closed her speech with some final advice to a group pursuing Singh’s vision of “choosing to carry [justice] forward.”
“Remember your motives,” she concluded. “Be patient. Build trust. Play the long game. Steward your degree with humility.”
Gallaga had attended the University of the Philippines Conservatory of Music in Diliman as a voice major, while belonging to the Philippine Madrigal Singers, an a capella choir that took her around the world for festivals, world tours, and competitions.
When Michelle Gallaga moved to the U.S. from the Philippines with her two young kids in 2010, she didn’t know anyone in her new home.
“We had to start a life and really try to navigate being an immigrant and all the hardships that come with it,” she says.
“When you move to a different country at 40,” she adds, “people already have their own friends and their cliques, and so I never really got to form my own group of friends.”
Not having completed college, she found, limited her opportunities, and she encouraged her kids to pursue the degree she hadn’t attained. Once they had left home to do so, however, it didn’t sit quite right with her that she had pushed them to do something that she herself hadn’t been able to.
And so, as a birthday present to herself, Gallaga enrolled at Berkeley City College, and not without some apprehension.
But it wasn’t the first time that the graduating Global Poverty & Practice student had enrolled in college.
Gallaga had attended the University of the Philippines Conservatory of Music in Diliman as a voice major, while belonging to the Philippine Madrigal Singers, an a capella choir that took her around the world for festivals, world tours, and competitions.
She spent seven months away from the Philippines during the group’s 1989 tour and found it difficult to re-enroll in classes after returning, choosing to stay on with the choir for another three years.
She eventually did go back to school again, this time for music theory, but dropped out after joining a cover band.
In 2000, Gallaga got married, retired from singing, and gave college another shot, studying education to become an elementary school teacher. For two years she taught English in rural schools with poor infrastructure and limited educational resources.
“I loved the experience of being there and being around the enthusiasm of the children,” she said. “It was so fulfilling and so humbling. There was something about giving yourself to it that you get so much out of.”
But a divorce brought an end to the calling she had begun to develop, and she had to drop out again. Eventually, she moved to the U.S.
Now, years later in Berkeley, Gallaga was quickly discovering that she loved being back in the classroom.
With so much more life experience to apply to her lessons, the curriculum clicked in a way it hadn’t before. In 2023, she transferred to UC Berkeley to study sociology.
But making the most of her time at the country’s top public university was difficult while working two jobs: one providing translation and interpreting services for San Francisco government agencies, and another assisting a social entrepreneur pushing for equity in the psychedelics space. She could only attend class two days a week — not enough to build relationships or finally find community.
That is, until she met Valerie Moss, the Blum Center’s Assistant Director of Student Affairs, at a Global Poverty & Practice minor tabling session on campus. Examining and addressing poverty immediately struck a chord with Gallaga and harkened back to her experience teaching students in underserved schools.
Its lessons about understanding 20th-century development and 21st-century poverty alleviation left her feeling like “I was living a lie all my life,” she laughed.
This is it, she thought during that first semester in the minor. I want to learn more.
Her biggest lesson, she said, has come this current semester. She had arrived at GPP believing that the only way to make a difference in poverty alleviation was to do work that produced obvious, immediate results.
“Joining the minor was the smartest thing to do,” Gallaga said, “because GPP gave me the community that I needed to really feel like I belonged at UC Berkeley.”
For her practice experience, a core component of the program where students apply what they learn, Gallaga volunteered with Spiral Gardens, a small, nonprofit community garden providing fresh, nutritious produce in a historically redlined Berkeley neighborhood and food desert — a place she herself had lived in for 10 years.
Gallaga at Spiral Gardens (courtesy photo)
Each Sunday, she would give tours of the garden to new volunteers, helped them get their own small garden projects off the ground, and mentored them. She grew food for her geographic community and gained the social community she had spent years looking for in the Bay Area and had begun to find in GPP.
Volunteering with Spiral Gardens also put into practice the lesson Prof. Kadir had imparted. Her biggest takeaway from GPP, Gallaga said, was “that I was there. I was a part of something. I did what I could, and I’ll keep doing what I can. And that’s enough. That’s what matters.”
After graduating this month, she plans to stay in the poverty-alleviation and nonprofit space. “Being able to keep working with organizations that help other people will always make me feel like I belong,” she said.
Her son graduated from UC Irvine in June, and her daughter will graduate from UC Santa Cruz next June.
“When I told my son, ‘I got into UC Berkeley!’ he was so jealous because he got rejected from Berkeley,” she recalled with a laugh. “But when I told him I got in, he said, ‘Mom’s the GOAT!’” — the greatest of all time.
And come December 20, when Gallaga crosses the stage to receive her diploma, they’ll be there to celebrate her degree.
Together, the cohort brings experience spanning data science, medicine, material science, policy, and more, and will spend the next 15 months in an intensive program that blends technical training with human-centered development courses — preparing them for careers in social impact, entrepreneurship, design, and sustainability.
Longyu Gong
When Longyu Gong describes life in Shanghai, China, she doesn’t just talk about the scenery but about connection, or rather, the lack thereof.
“It’s a very beautiful, modern city,” Gong said. “But people aren’t interacting with their neighbors or building an identity together.”
She would know — she studied urban communities at Tongji University in Shanghai, a city of more than 20 million residents that moves as quickly as it grows. The skyline is sleek and the streets are busy, but daily life, she explained, often feels disconnected.
Some of that, Gong believes, comes from the stress of work, but more deeply, it’s about design — the structure of the city itself isn’t made to encourage people to communicate or spend time together.
Skyline of Shanghai Pudong at sunset
That absence of connection, Gong believes, is as much an engineering problem as it is a social one, and it’s what brought her to UC Berkeley’s Master of Development Engineering program.
This August, Gong joined 27 fellow students at Blum Hall to kick off orientation for the fifth-ever cohort of the MDevEng program.
Together, the cohort brings experience spanning data science, medicine, material science, policy, and more, and will spend the next 15 months in an intensive program that blends technical training with human-centered development courses — preparing them for careers in social impact, entrepreneurship, design, and sustainability.
Between introductions, group exercises, and the occasional jet lag, students heard a recurring message from orientation speakers like Blum Center Faculty Director Dan Fletcher and DevEng chair Kara Nelson: pursue curiosity and take charge of your own learning.
“Berkeley is very much a university where initiative and self-motivation get you the most,” Fletcher said. “Berkeley is very much a smorgasbord, a buffet, and you need to figure out what it is you’d like to learn and what experience you’d like to have.”
The vital work of Development Engineering has grown more challenging and more essential in light of recent federal funding cuts and shifting government policies that have affected academia as a whole, according to Fletcher.
During the orientation, he addressed these challenges upfront, reminding students that there will always be a need for their work, even as newfound obstacles arise.
“The work we’re trying to do here is aimed at making the world a better place,” Fletcher said. “The needs are there, and the ability of each of us to make a positive impact is still there, so we can’t be dissuaded.”
His message resonated with the new students, many of whom are already eager to apply their skills to pressing global issues. Among them is Noam Anglo, who plans to focus on Healthcare Transformations during his time at Berkeley.
Noam Anglo
Born in the Philippines and raised in Canada, he studied mechanical engineering at the University of Calgary. In the years that followed, he moved through industries as varied as healthcare, robotics, and entrepreneurship, yet something about the work felt incomplete.
“I’m an engineer and I want to do engineering, but I just needed to figure out how to apply that in the context that is most meaningful to society,” Anglo said.
That search for meaning brought him to Berkeley. Building on his roots in the Philippines, Anglo hopes to work with underserved communities around the world — from Southeast Asia to sub-Saharan Africa — and to find ways for technology to “distribute power to individuals.”
None of the other programs he considered offered the blend of technical rigor and social purpose he was looking for, until he found Development Engineering.
At Berkeley, Anglo hopes to explore new fields such as agroecology and sociology, while also studying sanitation systems with Prof. Nelson, an expert in safe water and sanitation for resource-limited environments. He sees the MDevEng program as a place to learn how engineering can directly solve humanitarian problems around the world.
Anglo said the community has already made an impression, as he issurrounded by classmates who take initiative and think big — an environment radically different from the one during his undergraduate years.
The energy, he said, has pushed him to aim higher and see new possibilities for how engineering can serve society.
“Even in the week before classes, I’ve met so many people who are really stubborn and try to think long term about the social impact they can make in their careers,” Anglo said. “I want to meet more of those kinds of people.”
Sharing that drive is fellow MDevEng student Alejandro Rodriguez, who is equally passionate about bridging the gap between technical innovation and social impact.
Alejandro Rodríguez
With a background in biomedical and industrial engineering from the Universidad de los Andes in Colombia, Rodriguez said he began to notice a troubling disconnect between the priorities of the engineering industry and the real needs of the communities affected by its work.
He emphasized that technical expertise alone isn’t enough to address society’s most pressing issues; engineers must also grasp how their work impacts society, politics, and people’s daily lives.
That conviction is what ultimately led him to the MDevEng program, where technology and social impact meet by design.
“I think that this program really cares about its application and how we impact society,” Rodríguez said. “It really cares about how we can help.”
As part of the program, he hopes to strengthen his skills in technology tools and policy intervention, and is particularly interested in using data to understand real-world social dynamics through his chosen concentration, AI & Data Analytics for Social Impact.
Rodríguez, alongside the rest of the new cohort, will spend the next three semesters tackling technical challenges, collaborating across cultures, and working on community-driven projects — culminating in a summer internship and a capstone project that puts their ideas into practice.
With opportunities to test those ideas through initiatives like the Blum Center’s Big Ideas Contest, students will take what they learn in the classroom and apply it to social and humanitarian projects around the world.
“You’re embarking on a journey,” Fletcher told the cohort. “We hope to empower you to make the kind of positive change that you want to make in the world.”
Initiated by the American Indian Higher Education Consortium (AIHEC), the Alliance’s “backbone,” the collaboration opened doors for Berkeley students to intern at NTU, teaming up with faculty and peers on engineering projects in a month-long program in Crownpoint, New Mexico.
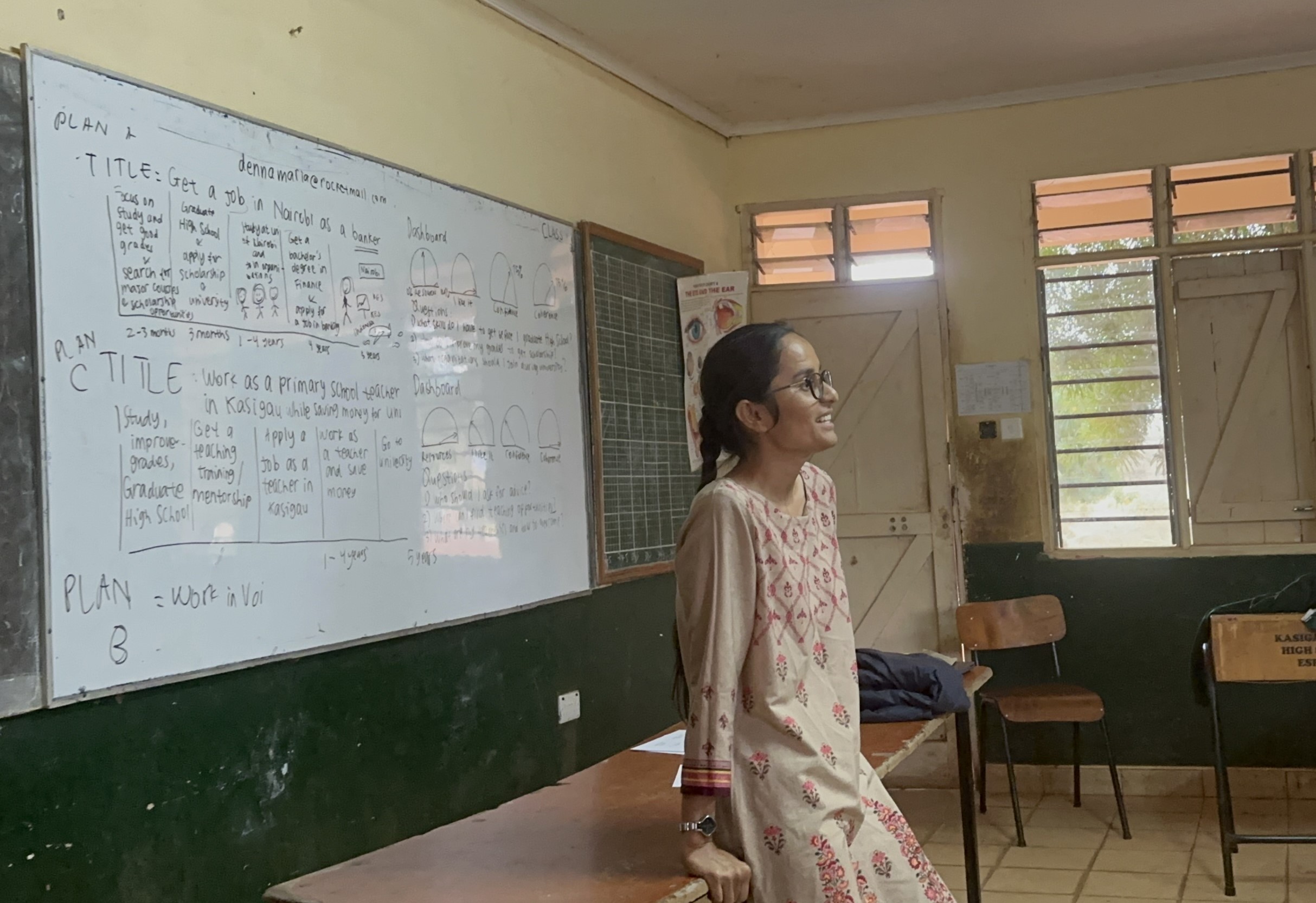
This past summer, UC Berkeley School of Education Ph.D. student Jessica Benally returned to the high deserts of her youth in New Mexico, just an hour away from her childhood home in Tohatchi in the Navajo Nation.
As one of six UC Berkeley students invited to take part in a new groundbreaking partnership program at Navajo Technical University (NTU), she set out to bring Navajo (Diné) culture into the classroom.
By combining Diné astronomy with mathematics, her doctoral project offers students a new way to learn math: looking up at the stars.
“In some math textbooks, students used the image of a ferris wheel that’s half above ground and half below ground (to understand angles),” Benally said. “But a ferris wheel, half above the ground, is not something students really see, so how about using an example of something that they can actually see?”
For her, the answer lies in the skies, where the rotations of Diné constellations like Náhookos Bi’ka’ (Ursa Major) and Náhookos Bi’áád (Cassiopia) seasonally rotate around Náhookos Biko’ (Polaris) reflect the 90-degree increments of the unit circle.
This type of visualization, she said, made math more accessible in her own childhood, and the insight inspired her to start work on STARR, or the Students Tracking Angular Rotation Recorder — a learning tool for teaching students about angles using their bodies and Diné star knowledge.
Beyond studying shapes on a piece of paper, students move their arms and bodies to create and measure angles while “traveling” across constellations in a small planetarium.
Over the summer, she would get the opportunity to further develop the model in New Mexico as part of her internship at NTU, offered through the collaboration between UC Berkeley’s Development Engineering (DevEng) programs and NTU’s Electrical Engineering (EE) program.
The six students part of the summer partnership program — including Benally and five others from the MDevEng program — were invited to NTU’s campus to work with faculty and fellow students on a variety of engineering projects, ranging from solar energy to air quality monitoring.
“In DevEng, we think a lot about under-resourced communities globally, but there are a lot of communities within the U.S. that are also marginalized,” UC Berkeley DevEng Director Dr. Yael Perez said.
“Being able to work with these communities, who are rich in culture but have limited access to other resources, and be part of their daily life for a short period of time, was a powerful experience, especially for students who come from other rich cultures who experienced marginalization elsewhere.”
The partnership took shape back in 2022, when Perez and NTU professor Peter Romine presented the idea of a joint engineering curriculum for Native American students at the American Society for Engineering Education (ASEE) conference in Minneapolis.
Perez, who also serves as the program coordinator for the Native FEWS Alliance — a cross-institutional initiative to expand participation in Food, Energy, and Water Systems (FEWS) education to all students, including Native Americans —helped put their vision into action.
Initiated by the American Indian Higher Education Consortium (AIHEC), the Alliance’s “backbone,” the collaboration opened doors for Berkeley students to intern at NTU, teaming up with faculty and peers on engineering projects in a month-long program in Crownpoint, New Mexico.
Students in the program stayed in the NTU dorms, and spent their time outside of engineering exploring the Navajo Nation and learning more about the culture from school staff, according to Kathy Isaacson, Native FEWS Program Coordinator at AIHEC.
“The six students from Berkeley really hit the ground running when they arrived at Navajo Tech,” Isaacson added.
For Benally, the partnership provided a chance to further her work on STARR within the community she aims to serve.
The project’s main goal is to combine different epistemologies, a term referring to “ways of knowing” or the different frameworks we use to understand the world around us. Benally’s curriculum weaves together Diné and western epistemologies, encouraging students to approach mathematics “pluralistically” through cultural storytelling and scientific methods.
The model pairs two students together: one serves as the Sensor, using an arm protractor to “become” each star in a constellation, with their arms forming the rays of an angle. The other acts as the Navigator, using a digital compass to guide the Sensor to the correct star position. Together, they trace constellations such as the Navajo Big Dipper (Náhookos Bi’ka’), combining cosmology and computation to make math education more engaging.
Traditionally, the Diné people have looked to constellations to track seasonal changes that guide farming, ceremonies, and other aspects of life, while also using them to build cultural philosophies and traditions. Building on this legacy, STARR blends both — along with other mathematical concepts — to help students grasp angles.
Originally, Benally improvised her tools, using a standard arm protractor made with tape and plastic tubing. Through her internship at NTU, she was able to refine the design, learning how to 3D-print protractors and develop more user-friendly compass tools based on participant feedback.
Benally also worked with former NTU student Hansen Tapaha to create “outreach kits” for K–12 students, designed to spark interest in engineering and incorporate technologies used in STARR.
As part of her ongoing work on the project, Benally was able to host two demonstrations of STARR at NTU for local students and staff through the collaboration. She plans to continue collecting data for the project, with the goal of presenting a final product as part of her dissertation.
“It was really amazing to get guidance from faculty expertise,” she said. “Being able to see it put together was really beneficial to making design improvements that will help the participant experience.”
At its core, each internship offered Berkeley students the chance to learn alongside the communities and traditions their work aimed to support, a hallmark of the DevEng mission, which trains students to tackle the needs of underserved populations. The DevEng programs, which include both a master’s diploma and a doctoral emphasis, combine advanced technology training with human development studies, preparing students for technical problem-solving and cross-cultural collaboration on the world’s most pressing humanitarian issues. Perez emphasized that the NTU partnership allowed students to put these lessons into practice by listening to and working directly with underrepresented groups like the Navajo Nation.
“Institutions like NTU and other tribal and community colleges are deeply embedded within their communities, which makes them vital partners in any effort toward meaningful, place-based impact,” Perez said. “This really makes DevEng–NTU an exciting addition to the Native FEWS Alliance.”
Many students who participated in the program are still working on parts of their project, which may turn into capstones they can continue developing at Berkeley in the fall semester.
Following this summer’s success, Perez said that they plan to expand the partnership by bringing NTU students to Berkeley and potentially hosting a joint course between the two schools.
She added that they are also looking to extend the invitation to other universities as well.
“Native American communities are very rich in culture and history, and they know what they want to incorporate in their current lifestyles,” Perez said. “It was really great to be part of that conversation.”
For Benally, the summer at NTU was an unexpected homecoming — a return to the high desert where her love for learning began, now enriched by the knowledge and perspectives she gained at UC Berkeley.
With support from the Blum Center, the Berkeley Lab scientist and his colleagues provided the first substantive analysis of how electric lighting — specifically, high-efficiency solar-powered electric light sources unattached to an electrical grid — improves the lives and well-being of people using fuel-based lighting.
After attending a conference on electric lighting efficiency in New Delhi, India in 1995, Dr. Evan Mills stopped by Varanasi for a vacation.
One night, he wandered through a car-free warren of alleys lined with shopkeepers. Standing against a wall in the marketplace watching humanity flow by, he had an epiphany — one that
A merchant in Varanasi, India using a kerosene lantern during a night market. (Photo by Evan Mills)
would help pave the way for the adoption of off-grid solar lighting on a wide scale.
“I look down to my left, and there’s a man with a blanket spread out, three feet by three feet. He’s selling bracelets and beads, and he’s got a kerosene lamp that’s lighting his wares, and everything’s sparkling,” Mills, then a scientist at Lawrence Berkeley National Laboratory, recalled. “And that was the proverbial ah-ha moment.”
At first glance, such lamps have an enchanting aura to them. But after that conference, Mills couldn’t help but wonder how much fuel the vendor was using, how much carbon dioxide was being released, how many others out there relied on this dim source of light to practice their business, and whether viable alternatives could be developed and brought to market.
“And then I started this odyssey,” he said, “that went on for decades to really try to nail that down.”
With support from the Blum Center and several other funders, Mills and his colleagues addressed a gaping hole in lighting research. They provided the first substantive analysis of how electric lighting — specifically, high-efficiency solar-powered electric light sources unattached to an electrical grid — improves the lives and wellbeing of people using fuel-based lighting. He calls it “wireless lighting.” They went on to create and implement international standards for such products.
Dr. Evan Mills with kerosene lamps and early solar lanterns collected for testing (courtesy photo)
GOGLA, an international organization that later picked up the mantle of this work, has reached about 140 million people in the developing world by supporting dozens of companies and investors. Non-profit groups such as Light Up the World also did pioneering work on this problem.
Fuel-based lighting, on the other hand, like the Varanasi merchant’s kerosene lamp, is associated with various health, environmental, and economic problems.
Beyond the difficulty in doing basic activities under such dim and inefficient light sources, they are fire and burn hazards and can wreck indoor air quality. They are orders of magnitude more expensive than fluorescent or even “inefficient” incandescent lighting, per lumen (a unit of brightness).
“A homeowner [in the U.S.] spends maybe five percent of their income on energy,” including for their car, house, heating, cooling, refrigeration and more, Mills explained. “A very poor person can spend five percent of their income on kerosene lighting alone.”
Under the Lumina Project, Mills organized his studies of off-grid lighting solutions for low-income communities around the world, as well as the provision of information and analysis to consumers, industry, and policymakers.
“He just gifted it to the Blum Center and said, ‘Here, do something good with it,’” Mills said.
That good funded the Lumina Project and other activities at the Blum Center.
“We were very lean and mean,” Mills said, applying the Center’s funding to equipment purchases, travel to countries for research, and supporting Berkeley students getting involved in the project. “We made the resources go really far.”
A huge area of research Mills and his team were able to pursue was market characterization and needs assessments. On the technology side, white LED lights had just been commercialized, which meant that by packaging small rechargeable lithium or nickel-cadmium batteries and tiny solar panels, one could create portable and affordable solar lanterns at a fraction of the cost of bulky incumbent systems. Miniaturization and pre-purchase assembly of components stood to be major breakthroughs.
Users of fuel-based lighting are “not a monolith,” Mills said. “It’s not just a kid with a lantern doing their homework.” It’s also a doctor treating patients in a clinic, a schoolteacher in a windowless classroom trying to light their chalkboard, fisherpeople on a lake at night, chicken growers, nighttime security guards, people in cottage industries, and women moving around refugee camps. How did all these people use light? What did they pay for it? What were their nuts-and-bolts engineering needs?
A night market in Kisumu, Kenya (Photo by Evan Mills)
From Kenya to India, Tanzania to Bhutan, Mills and his Berkeley students would take prototypes of portable electric lighting sources — which don’t require special expertise to set up — into communities and be peppered with questions by prospective users already well versed in issues around lumens and durability.
When a community’s health clinics adopted off-grid solar lighting, postnatal maternal mortality decreased, as did infection rates. At kerosene-lit night markets, the diverse colors of goods like flip-flop sandals would wash out into the same hue; under LED headlamps, the colors became immediately distinguishable — along with enough light for vendors to count change under the table. Unlike candles and lanterns, solar lanterns would keep working in the wind and rain, and users weren’t vulnerable to fuel shortages or price spikes.
The funding from the Blum Center also allowed students to spend weeks in Kenya and Tanzania to join night fishing trips on Lake Victoria.
Some 100,000 people go out onto its waters each night, Mills said, with kerosene lanterns floating on little rafts to attract the fish’s food sources, which allows fishers to draw the fish into their nets. But half their income from one night’s catch would go toward kerosene for the next night’s trip, keeping the people impoverished.
Mills and his team built prototypes of LED lamps, and the students spent night after night weighing fish caught with the kerosene and electric lamps and comparing the costs associated with both kinds of catches. The electric lamps essentially doubled their income. They got the same results on Lake Tanganyika and at sea.
Fishers on Lake Victoria using an LED lamp developed by LBNL and UC Berkeley students (Photo by Tim Gengnagel)
They also dug deeper into the health effects of fuel-based lighting: not just the worse indoor air quality and the deadly fires that kerosene lanterns can cause, but synthesizing the literature from doctors treating young children who had been burned by these lamps or had accidentally consumed kerosene. They learned that people who suffered medical emergencies at night often had to wait until daylight to be seen at a clinic, exacerbating their illness or injury and causing longer clinic lines for everyone.
Mills also shed new light on the scale and effects of kerosene subsidies ($35 billion annually), the potential for job creation with electric lighting, and the resources the latter required. They estimated that 150,000 jobs in the world involved kerosene lighting, but the widespread adoption of off-grid solar lighting could potentially produce two million jobs. They also figured out the energy and resources it took to make their LED lanterns and how long those lanterns would have to be used to make up for what was put in. (Twenty to fifty days for a device that would last years.)
There was, however, one snake in the garden. More and more companies were producing affordable, turnkey off-grid solar lighting devices. Mills’ team tested many of them and found considerable variability in the quality of their light output, batteries, wiring, and more.
“Eventually the World Bank got a whiff of this,” Mills said — specifically its International Finance Corporation. Mills helped them develop a successful proposal to the Global Environmental Facility (GEF) to scale up a market-transformation effort.
Mills brought aboard Arne Jacobson of Cal Poly Humboldt’s Schatz Energy Research Center, who, while a PhD student in Cal’s Energy and Resources Group, had studied why older solar lighting systems — featuring big panels, long fluorescent tubes, and heavy car batteries that required an electrician and a year of income to buy — hadn’t been widely adopted. Virtually every obstacle could be overcome with the emerging compact LED systems.
Building on that work, the Berkeley Lab–Humboldt collaboration helped IFC develop test procedures and create a quality-assurance program. At the core was a product-certification program (today called VeraSol). Companies took to it quickly, Mills said, learning how to improve their products. And a warranty and truth-in-advertising component was essential to prevent market spoiling: users having a bad experience with a deficient product and giving up altogether on off-grid electrical lighting.
The momentum for off-grid lighting kept building. A regular conference, organized by IFC, attracted people from dozens of countries, including environmentalists, government officials, and investors. A vibrant, online social network was set up where folks around the world shared insights and innovations, troubleshooted issues together, and found community. As a sign of the gradual mainstreaming, television soap operas in Africa depicted people purchasing solar lanterns.
Eventually the United Nations took note.
The UN Environment Programme wanted to know the carbon-offset value of using a solar lantern, and commissioned Mills and his colleagues to develop a methodology the UNEP could use to evaluate the use of solar lanterns in carbon markets. Their methodology’s adoption came at a critical time given what had been learned about the variability in product performance and quality.
Despite all the success, Mills said, the World Bank and IFC did not intend to stick with off-grid lighting indefinitely, and the movement needed a new organization to continue carrying the torch.
Its proponents founded the Global Off-Grid Lighting Association, which shortened its name to GOGLA once it expanded to include compact and portable solar home kits that made solar energy services more affordable and useful beyond just lighting. GOGLA now assists the off-grid solar community with finance, consumer protection and standards, market insights, advocacy, policy, and more.
Mills, now retired from Berkeley Lab, has moved on to work on other problems. When he started this work, over a billion people lacked electricity. Some 140 million people across the developing world now benefit from the improved products, with about 7 million solar lanterns and multi-light kits and 1.6 million full solar home systems sold each year.
Berkeley students were essential to collecting the data that became the backbone of what the off-grid industry has become, Mills said. As was the Blum Center’s flexibility.
“Complex undertakings like this do take time, and they take patience and dedicated sponsors,” he said. “The Blum Center generously provided us with a lot of trust and latitude to be nimble and respond to new ideas and opportunities.”
“It was so exciting because it was such a green-field area,” Mills added. “There were other people who were poking at this, for sure. But we were right there at the beginning, and the Blum Center was right there on the ground floor with us.”
World Water Week is an annual conference and global observance focused on tackling the world’s most pressing water-related challenges — urging policymakers and innovators to take bold action on sustainable solutions. This year’s theme, “Water for Climate Action,” highlights the essential role that water plays in reducing greenhouse gas emissions and adapting to a changing climate.
World Water Week is an annual conference and global observance focused on addressing the world’s most pressing water-related challenges — calling on policymakers and innovators to take action on sustainable water solutions.
This year’s theme is “Water for Climate Action,” which aims to address the crucial role that water plays in global efforts to reduce greenhouse gas emissions and the effects of climate change.
To understand how water-infrastructure innovations can combat poverty and address a changing climate, we spoke with Prof. Kara Nelson, a water infrastructure expert who also serves as the chair of the Development Engineering programs.
Prof. Kara Nelson
What water-related DevEng projects are you working on right now?
One of the biggest threats to clean drinking water in the world is the unsafe management of human waste, because a majority of the planet still doesn’t have access to safe ways of disposing of their fecal waste.
We’re trying to work at one of the root causes of the problem, so we’re working on strategies to collect, contain, and process human waste to then actually create value with it.
One of the ways we can do that is through a really cool toilet design which separates urine and feces. We can then take the urine and make fertilizer from it.
In a lot of regions of the world, fertilizer is also in limited supply — either because of a lack of availability or because it’s not affordable — so through this project, we can create a local fertilizer product that farmers can use to increase crop productivity.
The main place that we’ve been working to understand the practical aspects and feasibility of this approach is in Kenya.
Why do so many parts of the world still struggle to access safe drinking water?
We think that this approach to capturing urine and producing fertilizer from it can make sense in high income, as well as middle and low income contexts around the world.
What communities would this project be serving?
There are easily a billion people in the world that this solution could work for, but it would very much need to be adapted to the local context.
For example, we’ve been designing the full solution for a context like San Francisco, where people rely on flush toilets. We’re thinking about the technology needed for making the fertilizer that would be designed for spaces like the basement of an apartment building in the Bay Area.
So this is a solution that I think can be appropriate for any community in the world, but things like the user interface are going to be designed specifically for the local context.
This year’s theme for World Water Week is “Water for Climate Action.” How does your project aim to combat climate change?
This sanitation research has many ties to climate change, and it’s trying to address different dimensions of the climate crisis.
One of those dimensions is that if we could produce fertilizer locally from human waste, it would mean that farmers could use less synthetic fertilizer, and synthetic fertilizer is one of the most carbon-intensive products in the world.
All of the fertilizer that’s currently made makes up about two percent of the carbon footprint in the world, so if we could eliminate the production of that synthetic fertilizer, it would reduce global carbon emissions by two percent, which is huge.
Another dimension is that in communities across the world without access to flush toilets, developing waterless solutions — through nonflush adaptations of our solution — that are acceptable to users offers a great way to address growing water scarcity.
Because of climate change, more and more of the world’s population is going to live in regions with severe water scarcity, and one of the most water-consuming activities in the United States is flushing toilets.
We take water that’s of drinkable quality, and we flush it down the toilet. If we can develop solutions for sanitation that use no water or use less water, that is going to help us adapt to a dryer and warmer climate.
As DevEng chair, what role do you see Development Engineers playing in the push for climate action?
We always need to be thinking of ways in which any type of water infrastructure contributes to the climate crisis. We need to be asking ourselves how we can reduce those impacts, and then, how we can also develop infrastructure that is adapting to a changing climate.
Water solutions for conditions we have today may not be adequate 10, 20, or 50 years from now, so we need to be planning for the inevitable.
Even if all of us were able to eliminate carbon emissions today, there’s enough momentum from all the historical greenhouse gas emissions that the climate is going to change, and the most marginalized are going to experience the greatest impacts from climate change.
So, we really need to be prioritizing solutions for vulnerable communities around the world, and that’s part of the framing for our Development Engineering programs and curriculum.
As this year’s Global Poverty and Practice (GPP) graduates stepped onto the stage to receive their diplomas, they carried with them a hard-earned insight: the injustices they spent years studying weren’t distant or theoretical — they were urgent and unfolding all around them. Their time in the program has prepared them to enter the world beyond Berkeley with a strong sense of purpose, ready to confront poverty in a time of growing global uncertainty.
As this year’s Global Poverty and Practice (GPP) graduates stepped onto the stage to receive their diplomas, they carried with them a hard-earned insight: the injustices they spent years studying weren’t distant or theoretical — they were urgent and unfolding all around them. Their time in the program has prepared them to enter the world beyond Berkeley with a strong sense of purpose, ready to confront poverty in a time of growing global uncertainty.
Earlier this month, friends and family filled Sutardja Dai Hall’s Banatao Auditorium to celebrate the commencement of the GPP minor’s Class of 2025, the 18th cohort of students to tackle poverty by studying the global systems and power structures that sustain inequality.
Director of the Global Studies Program and Chair of the GPP minor Elora Shehabuddin spoke to the significance of this historical moment, with graduates completing their coursework, she said, amid escalating climate disasters, emerging armed conflicts, and the first livestreamed genocide, carried out by the Israeli state against the Palestinian people.
“In every case, you learned to read and think beyond the headlines of mainstream media, to consider the histories of these conflicts and the power dynamics that shaped them, and to center the history of the human beings affected,” Shehabuddin said. “These graduates inspire all of us as champions for social justice, and they represent the best of UC Berkeley.”
This year’s graduating class includes over 30 students representing more than 20 majors. As part of the minor, students completed a personalized practice experience that involved interning or volunteering with a government agency, nonprofit organization, or community group working on poverty issues.
A defining element of the program, the practice experience is designed to help students bridge theoretical frameworks with real-world poverty action, and it held particular meaning for student commencement speaker and legal studies major Johnna Spikes.
Johnna Spikes (Photo by Amy Sullivan)
With a family history rooted in public service, Spikes spent much of her early life engaged in similar work. She pursued a career in law, working as a paralegal and office manager at the law firm of Haddad and Sherwin. At Berkeley, she deepened her commitment to justice through internships with Legal Services for Prisoners with Children and the Ella Baker Center for Human Rights.
She joined GPP to continue her work in public service, but what she learned reshaped how she approaches that work.
“I entered this minor with an idealistic desire to serve, as I believed that by helping those who are suffering, I’d be fulfilling some noble mission,” Spikes said. “I’ve come to realize that service without connection can become charity. True compassion doesn’t come from a place of distance, it comes from standing shoulder to shoulder, seeing the humanity in each other, and walking forward together.”
She volunteered with Old Skool Cafe, a San Francisco restaurant run by formerly incarcerated, foster care, and at-risk youth. More than just a place to eat, the cafe operates as a violence prevention program, offering job training and meaningful employment.
At Old Skool, she saw firsthand how young people often pushed to the margins weren’t treated as problems to be fixed, but as leaders — shaping the menu, helping run the restaurant, and building the kind of community they wanted to see.
“That’s what love looks like when it is rooted in justice,” Spikes said. “In this work, compassion isn’t a gesture of service, it’s a radical act of kinship grounded in the belief that there is no us and them, only us. The fight against poverty and injustice isn’t just something we choose to do, it’s something we’re here for.”
Similarly, the minor challenged student speaker and civil engineering major Anahita Banerjee to dig deeper in her search for solutions to global inequality. She has extensive experience in global water access, and her fieldwork spans rural India, Peru, and California, where she’s partnered with local communities to develop clean, dependable water infrastructure.
Anahita Banerjee (Photo by Amy Sullivan)
As a GPP minor, she said her daily assignments challenged her to confront global issues by asking tough questions like, “Why is there a housing crisis in the Bay Area? Why does the U.S. have the highest incarceration rate in the world?”
She added that simple answers—blaming things like lack of wealth, infrastructure, or education—wouldn’t cut it. Instead, the program pushed students to keep digging until they uncovered the deeper systems behind these problems: a prison system profiting from forced labor, or policies that force formerly colonized countries to prioritize debt payments over vital infrastructure.
“Yet, I would still call these B+ answers at best, because our homework is incomplete if it remains passive,” Banerjee said. “The most important question that this minor instills in us is, ‘What are we going to do about it?’”
Driven by that same sense of responsibility, she plans to work as a reporter for a nonprofit covering water issues, and then pursue a master’s degree at the University of Oxford in Water Science, Policy, and Management.
Facing her classmates, she expressed confidence that they will all continue to ask these critical questions and strive to “earn that A+.”
“Some of us may continue working with nonprofits, while others will work as doctors, teachers, or social workers,” Banerjee said. “However, all of us will go on to be outstanding members of society and not allow ourselves to turn away from the injustices around us.”
The ceremony concluded with a speech from GPP alumnus Jamal Khan. He graduated as part of the second cohort of GPP students in 2009, and went on to attend Harvard Law School. Since then, he has held positions in both the federal government and politics, including the Obama White House and Kamala Harris’s Senate campaign. He currently serves as an attorney for The Homeless Action Center.
Jamal Khan (Photo by Amy Sullivan)
Drawing from his experiences in legal advocacy and direct support for unhoused individuals, incarcerated people, and those facing mental health challenges, he emphasized that dehumanization—whether in the language of war or in the bureaucracies of everyday life—is often the precursor to violence and neglect.
Khan left graduates with a powerful closing message:
“No matter the vantage point from your organization or your role, if you find yourself feeling uncertain or confused, the most important thing you can do with regard to those you’re trying to help, is to remember humanity,” Khan said. “Conågratulations, I wish you all the best. Go out there and do big things, go-getters.”
AgriSolar — a mobile and scalable solar-powered irrigation system designed for smallholder farmers’ accessibility and affordability — took home top honors and the first-ever Biggie trophy in the 12th annual Big Ideas Grand Prize Pitch Day on May 7.
AgriSolar — a mobile and scalable solar-powered irrigation system designed for smallholder farmers’ accessibility and affordability — took home top honors and the first-ever Biggie trophy in the 12th annual Big Ideas Grand Prize Pitch Day on May 7.
“It’s extremely exciting for the whole team that Big Ideas and others believe in this, believe in us, and are entrusting us with this award,” Raihan said. “This is a responsibility to do well.”
Read more about AgriSolar and this year’s Grand Prize Pitch Day here.
Ekta Raghuwanshi and Maria Denna, her MDevEng classmate, worked at A Better Education Club as part of an internship pilot program that DevEng and ABE Club look to expand in the coming years. The organization, based in Kenya’s southwestern region of Kasigau, supports youth education and women’s empowerment by focusing on health, food security, hygiene, and farming practices.
Ekta Raghuwanshi had a particular way of approaching challenges — professional, academic, and beyond: dive in, define and quantify the problem, produce a solution that fixes it. It’s an approach she learned from her background in software engineering — structured, analytical, and solution-driven.
Her summer internship at an education and poverty-alleviation organization in Kenya revealed the limits of that approach.
Raghuwanshi and Maria Denna, her Master of Development Engineering (DevEng) classmate, worked at A Better Education Club (ABE Club) as part of an internship pilot program that DevEng and ABE Club look to expand in the coming years. While Raghuwanshi’s technical problem-solving mindset was valuable, she quickly realized that local intricacies — social, cultural, and contextual — couldn’t always be captured through a purely technical lens. Adapting to these complexities required a shift in thinking, one that blended structured problem solving with a deeper, more nuanced understanding of local realities.
ABE Club, based in the southwestern region of Kasigau, supports youth education and women’s empowerment by focusing on health, food security, hygiene, and farming practices in this region of some 20,000 residents. Alex and Megan Isaacs founded the NGO in 2004 when they were high school students. ABE Club grew with the support of the siblings’ father, Steve Isaacs, a UC Berkeley alumnus.
Raghuwanshi was eager to learn from ABE Club’s 20 years of experience in Kasigau, exploring first-hand how the organization had made an impact and how the development lessons from her coursework played out in real-world contexts.
Denna, a Digital Transformation of Development fellow, had experience organizing a school club that sent volunteers abroad and had joined a leadership program during undergrad that focused on social impact. She went on to put her technical experience to work as a product manager in tech, but found she couldn’t apply her passion for social impact. The MDevEng program — a multi-disciplinary, context-driven field pioneered at Berkeley that produces solutions to problems in under-resourced communities with their participation — allowed her to combine that passion and technical expertise. And that, in turn, led her to ABE Club.
“In my personal experience, I’m torn between two worlds,” Denna said, “my technical, engineering-oriented classes and the more sociological ones exploring why otherwise sound technological interventions fail in under-resourced places. The ABE Club internship brought these two worlds together: How can we ensure that our technical skills, or the technical intervention we want to bring, actually fit the local context?”
Raghuwanshi in class (Photo by the school).
Teaching and learning
Over this past summer, Raghuwanshi and Denna stayed in Banda House, a cottage in one of Kasigau’s villages often used for children’s retreats. The interns were to understand the local community of Kasigau in order to advise on potential innovations.
One of their primary tasks was to perform a needs assessment of the community to see where there could be opportunities to work on innovations to improve community resources and infrastructure. Raghuwanshi wanted to see what previous projects and programs had occurred in their particular village — primarily infrastructure, like water tanks — and how the organizations behind them measured and thought about those contributions. The interns wanted to understand “the village as a system and the inner machinery of it,” Raghuwanshi said.
Balancing the need for thorough understanding with the urgency to make an impact posed a tough dilemma for Raghuwanshi. “Finding the right intersection of both was really important,” she said, as her internship required her to contribute meaningfully to ABE’s mission of empowering the community through education and technical solutions — within a limited timeframe. She came to experience firsthand what she had learned in her own classroom at Berkeley: This challenge is not unique. Many well-intentioned international organizations have faced the same dilemma, with some acting too quickly and unintentionally causing harm to the communities they aimed to help.
After performing their community assessment, Denna and Raghuwanshi moved into more project-based work and training. Denna, for instance, taught the basics of computer programming, life skills, career planning, reproductive hygiene, and boundaries. In her healthcare lessons, for instance, she explored managing pharmaceuticals for the local clinic, how to inventory them, and how to digitize those inventories through the available technologies.
At the end of the day, Raghuwanshi said, the goal was to “really understand the context and not push your assumptions on people” — not to parachute in and solve problems, “but learn from them what they want” help with and to be a partner in that, suggesting solutions that are accessible and to see what Kasigau residents want to adopt.
“Ekta and Maria did an amazing job,” said Joram Kapala, ABE Club’s operations assistant and staff writer. “They interacted with community women groups and community members dealing with a kitchen-garden program. It was so eye opening to see the creativity and resource utilization” within the groups.
“Interns looking for challenges and willing to suggest and test possible solutions with ABE,” he added, are an important way for the club to hit its near-term goals of improved food security, a 100-percent high school education-completion rate, equitable implementation of WASH programs, and full availability of essential medications at health clinics.
Denna teaches a computer programming class (Photo by Raghuwanshi).
Rethinking development
Raghuwanshi came away with a new perspective of what development looks like.
The internship allowed her to not only process the lessons she learned in DevEng classes like “Critical Systems of Development” but to become more reflective and introspective, thinking critically about her own role in a foreign community. Starting from a blank slate, without any assumptions and biases, and filling it in with the community and its specific circumstances and perspectives is the first step, she says.
In the one and a half months she spent in Kenya, she had initially pressured herself to come out of the internship with some sort of tangible deliverable.
“Maybe sometimes it doesn’t have to look like a technical deliverable,” Raghuwanshi said. “Maybe the ‘deliverable’ can look more like ideas that have changed and how we all have changed as people.” Such changes, like empowerment, aren’t necessarily measurable or quantifiable but can nevertheless lay the groundwork for future solutions self-implemented by the community or that the next generation of interns can co-implement with them.
The internship not only deepened the interns’ understanding of development work but also encouraged them to reflect on how organizations like ABE Club and its partners navigate long-term support for communities like Kasigau. Denna noted that some interventions can unintentionally create dependency on donors. The goal, she added, is to help foster greater independence and self-sufficiency, such as by expanding entrepreneurship opportunities in places like Kasigau, and examining the intersection of social, economic, and political forces in service of systemic changes that go beyond mere technical solutions.
Back in Berkeley, the DevEng master’s students carried these questions into their final semester, bringing them into discussions in their Development Engineering Ethical Reflection course, where they continued to grapple with the complexities of ethical and effective development work.
“It certainly shifted something in me,” Raghuwanshi said of the internship. “It made me ask all of those questions — and keep searching for better answers.”
Every summer, UC Berkeley’s Development Engineering students create global social impact. The 2024 DevEng Photography Contest showcased their work, highlighting projects from digital education in Kenya to climate justice in Nigeria. Winning submissions emphasized human-centered technology, community-driven financial practices, and sustainable development, capturing innovation and resilience through powerful visual storytelling.
Every summer, students in UC Berkeley’s Development Engineering programs set out to create social impact locally and globally, implementing community-centered DevEng initiatives that focus on underserved populations. During their summer internship experience, students learn to combine expertise in engineering, economics, entrepreneurship, natural resource management, and social sciences to design technology-driven solutions that tackle the most pressing challenges faced by low-resource communities worldwide.
2024’s DevEng Photography Contest invited students to submit photos and videos that show what DevEng means to them and to capture the impact of their work over the summer through creative media. The following submissions — from digital education initiatives in Kenya to climate justice efforts in Nigeria — highlight how technology, education, and community-driven financial practices are fostering more equitable and sustainable futures.
By Maria Denna, Master of Development Engineering. Concentration area: Sustainable Design Innovations.
Tailored Education
“The photo was taken during my internship in Kenya, where I taught digital skills and cybersecurity to the students. I also worked with the local government to digitize their clinics’ drugs inventory,” Denna said. “I saw the gap between how a technology or intervention was designed and how it was actually implemented in the context of rural Kenya. Therefore, I would like to highlight the importance of localizing technology and designing a human-centered intervention that encourages community participation.”
“Project-Based Learning in Action”
By Ekta Raghuwanshi, Master of Development Engineering. Concentration area: Sustainable Design Innovations
Project-Based Learning in Action
“In a beautiful mountainous village in Kenya, children gather under the vast open sky, which has become their classroom. There are no high-tech labs or fancy equipment — just the natural world around them and their own creativity,” Raghuwanshi said. “As part of their curriculum, these young learners are exploring project-based learning, a method that encourages hands-on experiences and real-world problem-solving. With the right support and guidance, this creativity can flourish, leading to a future where every child has the opportunity to learn, create, and thrive.”
“Holistic Growth: Systems Thinking and Community Empowerment”
By Ekta Raghuwanshi
Holistic Growth: Systems Thinking and Community Empowerment
Raghuwanshi’s photo features Angeline from Kasigau, Kenya, a member of a Table Banking initiative organized by Compassion Kenya. The organization focuses on child development and supports families by creating livelihood opportunities, including the promotion of table banking. She added that this community-based financial practice has become increasingly popular in rural Kenya, where group members combine their savings and lend the pooled funds to one another.
“Angeline owns a tailoring business — she stitches bags and school clothes — and now she wants to expand her business to create sweaters. She took $500 in loans from her table banking group to invest in a bigger stitching machine to start her sweater business,” Raghuwanshi said. “I included this specific photo because many images depicting women in African countries often evoke feelings of pity, focusing narrowly on their circumstances. Recognizing their dignity and individuality is the starting point of meaningful development work.”
Video
“Climathon Kano Project: Climate Conflict Mitigation for Sustainable Peacebuilding in Nigeria”
By Hussein Orekoya, Master of Development Engineering, Concentration area: Energy Waster and the Environment
“The Climathon Kano Project addressed the complex challenges at the intersection of climate change, natural resource depletion, and violent conflict in northern Nigeria,” Orekoya said. “It aimed to develop strategies for climate-induced conflict mitigation using the Rondine Methodology, a relational approach to conflict understanding, resolution, and peacebuilding. With financial support from Projects for Peace and the International House at the University of California, Berkeley, the project reached over 80,000 farmers, herders, and stakeholders across 10 local government areas in Kano State, Nigeria.”
At Berkeley’s 2024 Master of Development Engineering commencement, graduates like Tilti Thind and Excellence Joshua celebrated transformative journeys. Their capstone projects and unwavering commitment embodied Berkeley’s spirit of radical change. Amid challenges and sacrifices, they emerged as determined changemakers ready to address global inequality and build sustainable, equitable futures worldwide.
Titli Thind
Tilti Thind didn’t make the decision to become a changemaker overnight — it was a journey years in the making.
During the pandemic, she was among the pilots leading India’s Vande Bharat Mission evacuation flights, bringing citizens back from across the Middle East — mostly migrant workers trapped in exploitative conditions. But upon returning home, she saw similar images of suffering: India’s own migrant workers, left jobless by the lockdown, walking for days along highways to reach home.
The sight ignited something that had been brewing in her. After 13 years of flying planes, she decided to step away from aviation, despite the whispers of friends and family questioning her “madness.” With a newfound desire to unravel the systemic roots of inequality, she set out in search of pathways to justice, dignity, and development.
This passion set her on the path to becoming a Development Engineer, and she shared this snippet of her path to Berkeley with classmates and their families during the commencement ceremony for the Master of Development Engineering program’s Class of 2024 — the third-ever cohort of a world-class degree program
“As I look out at the graduating class of Development Engineers, I realize that I have found that familiar ‘madness’ that I now identify as passion, hope, and idealism,” Thind said during her graduation speech. “This is what I see as the fuel for the field of Development Engineering — the community of practice”
MDevEng students combine engineering, economics, business, policy, and social sciences to prepare for careers focused on social impact and sustainability. The program demands rigorous courses, a summer internship, and a capstone design project, equipping students with both the technical skills and theoretical knowledge needed to drive meaningful change. The 2024 cohort’s 31 students came from 11 different countries.
At Berkeley, Thind became a Big Ideas finalist for Narmadaई, a project that partners with communities displaced by India’s Sardar Sarovar Dam. Her capstone project explored the politics of Mumbai’s Salt Pan lands, examining how colonialism, political power, and migration shape the freedom of landscapes.
“It’s the dreams, the challenges, the excitement, the tears, the immense sacrifices, and the collective values that made us gravitate to a program disrupting the way development and engineering are practiced,” Thind said, referring to her peers’ urge to effect change in the bold, transformative spirit of Berkeley, an institution known for leading radical change.
Among this graduating cohort, many students were similarly driven by a shared commitment to creating transformative social change in their own communities, including fellow student speaker Excellence Joshua.
Excellence Joshua
Before Berkeley, Joshua founded Techy Train Incubator, a nonprofit dedicated to equipping African women with tech skills and connecting them to global opportunities. Since its inception, the organization has trained over 10,000 women across 35 countries, with more than 3,500 now outsourcing their talents on a global scale.
In her commencement speech, she reflected on initial worries about adapting to a new culture, managing the demands of a rigorous program, and on top of it all, raising her son as a single mother. However, she shared that the experience ultimately taught her that challenges are “stepping stones” for pursuing dreams.
“I felt like my dreams were too big for someone like me, but coming here to Berkeley reminded me that this was the very reason to dream even bigger,” Joshua said. “We are more than graduates: We are dreamers, we are creators, and leaders committed to building a future where equity, innovation, and change are tangible.”
At Berkeley, her capstone project focused on healthcare policy and helped to identify gaps in menopause care for women in the US and beyond. She concluded her speech by expressing gratitude to her peers for their support, contributions, and friendship throughout their 16 months in the program.
“I dare to say, I studied with the best minds,” Joshua said. “You challenged me and constantly reminded me that I wasn’t alone — all the friends who made late night deadlines a little more bearable with laughter and friendship.”
After sharing her own experiences in the DevEng program, Cherukumilli encouraged the cohort to tackle global challenges with confidence, even in the face of a rapidly changing world. Acknowledging the uncertainties ahead, she left graduates with a powerful message.
“To do work in the real world is both tough and rewarding at the same time, requiring you to develop grit, empathy, respect, humility, and patience,” Cherukumilli said. “I would encourage you to believe in yourself and never give up. Ever.”
We celebrate the life of Jimmy Carter, 39th President of the United States, and send condolences to his family and friends. As President, he advanced solutions to global conflicts, championed human rights, and promoted development. After the White House, he continued serving the world through the Carter Center’s impactful initiatives.
We celebrate the life of Jimmy Carter, 39th President of the United States.
We send our condolences to his family and friends — especially to our esteemed Trustee John Hardman, who served alongside him for over 20 years as CEO of the Carter Center.
As President, he worked to find solutions to international conflicts, to advance human rights and democracy, and to promote economic development. After leaving the White House, he continued this work at the Carter Center to “Wage Peace, Fight Disease, Build Hope” for people across the world.
Thank you, Mr. President, for a life well lived in service of others. We at the Blum Center continue to be inspired by your work.
Mingxi Tang, inspired by UC Berkeley’s Master of Development Engineering (MDevEng) program, shifted her career path from finance to social impact. Now part of the 2025 cohort, she aims to use AI and machine learning to improve the lives of people with disabilities.
Mingxi Tang studied finance at The Chinese University of Hong Kong, Shenzhen, and had plans to pursue a career in the industry after graduation. Her path took a sudden turn the day she discovered a video on the UC Berkeley website — an introduction to the Master of Development Engineering program.
The video showcased MDevEng professors working in under-resourced regions across the world, striving to improve the lives of people living in low-income communities using technology to measure soil nutrients for crop growth. Inspired by the various student projects she saw on the website, Tang applied, was accepted, and packed her bags for Berkeley.
“Honestly, I was really moved. I knew I had to apply to the program, because I wanted to learn the technical skills I need to help people live better lives,” Tang said.
Tang is now one of the 28 students that make up the fourth MDevEng cohort. The class of 2025 comes from all over the world, with students hailing from China, Uganda, Ireland, and beyond, and having academic backgrounds ranging from mechanical engineering to applied languages. On August 22, Tang met up with the rest of her classmates — each pursuing their own concentrations such as sustainable design and AI and data analytics — at Blum Hall for the start of MDevEng orientation.
“We’re all coming from different disciplines and communities, and now we’ll learn how to work together,” MDevEng Program Director Yael Perez said to the new cohort to kick off orientation.
The MDevEng program is a 15-month experience merging in-depth technology studies with human development courses to prepare students for careers in social impact, social entrepreneurship, and sustainability. Over three semesters, students engage in technical problem solving, cross-cultural collaboration, and community development, including a summer internship and a final capstone project.
Mingxi Tang (left) and Neel Simpson share their common interests during a bingo icebreaker activity. (Photo by Brittney Byrd)
During the reception for the incoming cohort, Blum Chancellor’s Chair in Development Engineering and Professor Kara Nelson offered advice on how to make the most of the three-semester program, drawing from her own career pathway to share her experience with students. Nelson described how she was often told to stick to a single field of study, reflecting on the limitations of engineering programs of the past.
“This program did not exist when I was a student. Professors would meet with me [about my project ideas] and tell me ‘you can’t do that!’ But today, we’re here to tell you that ‘you can do that!’” Nelson said. “You all have your own interests, your own backgrounds, and you know what your vision is. We’re here to support you and help you paint that path.”
Among the cohort, many students share the common goal of applying AI and emerging technologies to create sustainable solutions for improving quality of life. Tang, for instance, aims to develop her skills in supervised machine learning to create technology that can improve the lives of people with disabilities.
“I want to acquire a lot of skills during my time here and use my knowledge about AI and machines to help improve people’s lives,” Tang said. “With the kind of experience this program can offer me, I feel like I can definitely achieve that.”
Throughout orientation, many students vocalized similar aspirations to serve underprivileged communities, among them Pratiyush Singh, a Berkeley graduate who studied civil engineering and is passionate about addressing climate adaptation and water quality issues in India and Africa.
After two years in industry, Singh saw a disconnect between his work and the communities he aimed to serve. This pushed him to apply to the MDevEng program, where he wanted to employ his expertise in a more impactful way. Singh found the program unique in that it allowed him greater control over the kind of projects he would work on, and a focus on practical application rather than traditional learning methods.
“Through this program, I want to learn more about using AI and data to scale technologies for low-resource communities,” he said. “I’m going to continue my past work that focused on addressing water quality challenges, and hopefully I’ll improve along the way.”
The new cohort got to know campus through a scavenger hunt. (Photo by Brittney Byrd)
During orientation, students participated in an activity where they answered what Development Engineering meant to them using a single word. Common responses displayed on the projector screen included “sustainable,” “solutions,” and “community.” However, Singh’s choice of the word “minority” stood out to the cohort.
“I think of it as justice engineering at the end of the day, because the solutions we’re creating are taken to and impacting minority communities,” Singh explained. “I feel like when you address those problems, it’s a form of social justice.”
Orientation concluded with an alumni panel featuring Morris Chang, Kaavya “Kavi” Reddy, and Kangogo Sogomo from previous MDevEng cohorts, followed by a social mixer that brought together past and current cohorts, as well as MDevEng faculty and staff. It was the first event of its kind for an MDevEng orientation.
Reddy, an alum from the first MDevEng class, invited students interested in working with climate change and government organizations to talk to her during the mixer and exchange ideas. Now working with the science-entrepreneurship nonprofit ACTIVATE, Reddy, who started her own concentration while at Berkeley, encouraged the class to pursue projects they were passionate about.
She concluded with a powerful piece of advice: “Take Development Engineering and make it work for you!”
She elaborated, “If you go out [into the workforce] and you’re not really sure where you fit in [as a DevEnger,] then you’re feeling exactly what you’re supposed to,” Reddy said. “We’re so brand new that we’re bringing this entire discipline to the world.”
Kevin Kung, co-founder of Takachar, began his climate innovation journey at UC Berkeley’s Blum Center through the 2015 Big Ideas Contest. Now hosting California Climate Action Fellows, Takachar helps transform agricultural waste into bioproducts, emphasizing a human-centered approach that addresses environmental challenges and supports underserved communities.
Kevin Kung has worked with Berkeley and the UC system for a long time.
He and the social enterprise he co-founded, Takachar, which converts agricultural waste biomass into useful bioproducts, worked with Lawrence Berkeley National Laboratory through its Cyclotron Road fellowship for entrepreneurial innovators (now called Activate). Kung and Takachar went on to partner with Berkeley faculty and worked with various campus competition and internship programs.
But their beginnings in climate innovation were at the Blum Center.
“Our experience with the Blum Center actually goes back to 2015,” he says. “They were the first in the UC system to actually give us funding, through the Big Ideas Contest.”
Kung went on to win that academic year and got an up-close view of the breadth and depth of social-impact work facilitated by the Center. Nine years after joining Big Ideas@Berkeley, Kung and Takachar are returning the favor, now as a fellowship host through the California Climate Action Fellowships, a UC Berkeley program launched by the Blum Center and funded by a grant from the UC Office of the President and California legislature that pairs students with public agencies, private sector entities, community-based efforts, and non-profit organizations to support projects serving communities that are most vulnerable to climate change.
“We always enjoyed and were really inspired by the different projects the Blum Center has done,” Kung says. “We see this fellowship as another way to deepen that affiliation and also potentially provide an educational experience for students who may be looking for climate- and climate justice–related topics and can work at our site locally.”
‘Fighting for your children and your grandchildren’
For all the dangers that climate change has started unleashing on our planet — sea level rise, catastrophic weather events, invasive animal migrations — Daven Northroup-Kuder does not worry about the Earth’s future.
“The world will be fine; life will continue on,” the recent Master of Engineering graduate says. “It’s been through mass extinctions before.”
For Northroup-Kuder, who recently finished his Climate Action Fellowship with Takachar, it’s the human stakes — the impacts on those we care about, the consequences we can all relate to — that hit home the urgency of stopping the climate crisis.
The reactor Northroup-Kuder worked on during his fellowship (courtesy photo)
“You’re basically fighting for your children and your grandchildren and your great-grandchildren,” he says. “Making sure they don’t have perpetual asthma for their entire lives and having to breathe out of a respirator; having access to fresh drinking water and getting to see the beautiful ecosystems that you got to see.”
Before joining UC Berkeley, where he pursued business-focused bioengineering with an emphasis on synthetic biology, Northroup-Kuder studied microbiology and oceanography at the University of British Columbia and conducted research projects in fields ranging from molecular biology to geomicrobiology.
But in carving out a path where he could make meaningful contributions toward ensuring a prosperous future for humanity, he grew disillusioned with what he saw as a disconnect between academia and what happens on the ground, away from ivory-tower labs and classrooms. And government, he believes, can be a little too slow in effecting the change needed now.
He found the ideal middle ground via a social media post: The California Climate Action Fellowships was selecting its inaugural cohort of student fellows. In April, Northroup-Kuder started as a project engineer at Takachar.
‘Catalysts for driving innovative solutions’
Takachar tackles agricultural waste biomass: think the husks and cobs of corn that have no immediate use once the kernels are harvested. All that stuff has to go somewhere, and in many places, composting isn’t an efficient or realistic option. Plenty of farmers have resorted to simply burning this waste where it’s made.
Takachar produces small-scale tech and portable equipment that allows rural communities to self-sufficiently transform all this leftover crop and forest residue into bioproducts like nutrient-rich fertilizers, which come with a host of benefits for the health of these communities’ soil, crops, and surrounding ecosystems. The now-charcoalized waste reduces pollution and fires, while capturing carbon in a more durable form that decays more slowly than just composting.
“What’s unique about the fellowship program is it’s open to master’s students, who certainly bring another layer of experience that we normally don’t see,” says Kung, now Takachar’s CTO.
Takachar’s equipment converts agricultural waste biomass into useful bioproducts like fertilizers. (Courtesy photo)
Students, with their fresh perspectives and indefatigable drive, are the “catalysts for driving innovative solutions to age-old challenges like food insecurity, health disparities, climate change, and poverty,” says Big Ideas director Phillip Denny. “Their ability to see the world through a new lens allows them to tackle these issues in ways that others may not have imagined or dared to pursue.”
By equipping students, Denny adds, with essential early-career resources — mentorship, skill development, even seed funding — “we’ve witnessed time and time again how their ‘big ideas’ can create a profoundly positive impact on individuals, communities, and our planet.”
Northroup-Kuder arrived at Takachar excited to join the team and to get to work in a wide variety of areas, some of them new to him, recalls operations lead Rod Kux.
“He showed really good interest and actual hands-on experience when we needed him, which was very refreshing,” Kux says, “He’s experienced; it’s not his first rodeo. He’s done a lot in his life.”
While finishing up his graduate classes, Northroup-Kuder put in two-to-three days a week on-site in Sonoma County, where the company is in the final stages of developing a bigger version of its equipment, which it plans to have on the market early next year. (Its existing model is already deployed in India.) As a project engineer, Northroup-Kuder would prototype and repair the machinery (wherein temperatures can hit 900 degrees Celsius), handle logistics, and jump on a variety of smaller side projects as they arose. He would load in the biomass one day and brainstorm ways out of technical hiccups the next.
“This experience has really taught me how important it is to actually get out in the field and practice stuff. I just can’t understate the importance of building the thing and getting out in the world and testing it,” he says. “You can do all these CAD designs and make it look perfect and pretty, but no plan survives first contact — in this scenario, first contact with the real world.”
‘A human-centered approach’
And getting out onto the front lines isn’t just about the technology, but also those for whom the technology is made, particularly end users in underserved communities.
“It’s not necessarily, ‘Let’s just build a state-of-the-art gadget and ship it in and hope for the best,’” Kung says. “But taking a human-centered approach and saying, ‘What are the most urgent needs and desires of the end users and prospective customers?’ How do we work with them to understand that and listen to them and their stories, such that when we do the engineering, we have those in mind and even have a collaborative, co-design process?”
Takachar asks many of its employees, regardless of job function, to work out on the front lines “because it’s really important to understand how that work gets into the bigger picture of environmental justice and climate justice, to understand how it’s really going to affect the people and be integrated into their lives,” Kung says. “That’s a skillset we’d like to see integrated into the next generation of the workforce.”
For Northroup-Kuder — part of the vanguard of that generation — the path to helping steer the future of our children, grandchildren, and great-grandchildren remains wide open. For now, he plans to work in industry and pursue climate-focused bioengineering.
“I really think the goal of creating a sustainable world,” he says, “will be built on the back of biotechnology” — a field he wants to make more accessible to more people.
“I’ve really been driven by that mission” to assure a healthy world for future generations, he adds. “The world needs help now. It doesn’t need help in 15 years when you finish up your publication.”
We are thrilled to welcome Dr. Doll as our new lecturer for GPP 115. This course serves students all across campus, introducing them to historical and contemporary debates on addressing poverty and inequality in the world. Dr. Doll’s extensive experience in the disciplines of critical development studies, political ecology, and cultural geography will bring a valuable perspective to this course.
It’s not easy — amid life’s various inflection points, large and small alike — to pinpoint one opportunity that reset the compass of one’s life trajectory. But Ross Doll recalls an experience that fits the bill.
Doll, a postdoctoral researcher in the Geography department, was an undergrad in English at Berkeley trying to fix his burnout from working too hard and grappling with heavy theoretical questions with even more hard work and academic dedication. “I started to feel very detached from the world around me,” he recalls. “Because I had lost all sense of perspective, I couldn’t solve the problems I was considering.”
As a senior, he joined a Berkeley School of Education program that trained undergraduates in tutoring youth who needed help with reading. “It mattered so much to connect with my student, to slow down to his pace and see the world from his perspective, and to make a small difference in his life,” Doll says. “I don’t think I could have articulated it at the time, but tutoring made my world feel bigger, grounded, and purposeful.”
“This program,” he adds, “saved me.”
His new perspective ultimately led to two years in Romania through the Peace Corps and six years working and studying in China. Amid a slew of academic publications, intensive Chinese-language programs, fellowships, and teaching appointments, Doll earned his master’s in China studies and Ph.D. in geography from the University of Washington. Now, the Ciriacy-Wantrup Postdoctoral Fellow in the Department of Geography can add lecturer with the Global Poverty and Practice minor to his extensive résumé. This fall, Doll will teach GPP 115: “Global Poverty: Challenges and Hopes.”
“I see the goal of the GPP minor as providing a grounded and community-focused experience,” he says. “So, GPP 115 appeals to me because it provides a kind of full-circle moment to encourage and help inform such engaged learning opportunities for current UCB students. I’m honored and thrilled to be a part of it.”
GPP 115 focuses on 20th-century development and 21st-century poverty alleviation, including popular ideas of poverty alleviation, the institutional framework of poverty ideas and practices, and the social and political mobilizations that seek to transform the structures of poverty. Doll’s research draws on critical development studies, long-term ethnography, cultural geography, and political ecology in his focus on agrarian change in Asia. His expertise includes understanding how history, place, and security — or insecurity — play into “the uneven geographies of development in rural China” under the government’s modernization of agriculture.
“We are thrilled to welcome Dr. Doll as our new lecturer for GPP 115,” says Clare Talwalker, GPP minor lecturer. “This course serves students all across campus, introducing them to historical and contemporary debates on addressing poverty and inequality in the world. Dr. Doll’s extensive experience in the disciplines of critical development studies, political ecology, and cultural geography will bring a valuable perspective to this course.”
For Doll, the deepest learning experiences happen when students can apply what they’re studying through their own experiences — “when what you’re studying seems relevant, applicable, and/or has personal stakes,” as he puts it.
Take corruption in Romania. The issue meant nothing to Doll before he moved there and got to know folks who suffered from the resulting income inequality and “a common feeling of resignation.” That inspired Doll to study the origins of that corruption, which included the role U.S. foreign policy plays — and by extension, “my own decisions, perspectives, and values.”
As well as seeing his Romanian neighbors as people like him, “I also came to care about the issue of corruption because I saw how I was complicit in its creation and maintenance,” he says. “Which was an awful realization, but also an empowering one, since I could see the role I could play in changing that situation.”
“Those two points of care and connection — to my friends and to my actions — self reinforced and encouraged me to dig deeper and to be more conscious of how I lived my life,” he adds.
By bringing those “points of care and connection” to the classroom, Doll believes students’ resulting sense of responsibility and empowerment will drive them to dig deeper into the ideas, problems, contexts, and solutions the GPP minor will explore, including through a hands-on practice experience.
“You start to see that not only can you not impose your values on [students] or tell them what to think, but there’s no need to, because that spirit of inquiry from the foundation of responsibility and empowerment will guide them,” he says. “And that kind of self learning is so much more powerful and lasting than any ideology or perspective you could try to articulate or impose anyway.”
Last month, the Global Poverty and Practice minor’s Class of 2024 celebrated a hard-earned and well-deserved commencement with an intimate ceremony in Sutardja Dai Hall’s Banatao Auditorium.
Finding success in college is not easy, particularly when you start at the height of a global pandemic. And doubly so when your studies entail a nuanced understanding of and unwavering willingness to act on local and global poverty and inequality.
Last month, the Global Poverty and Practice minor’s Class of 2024 celebrated a hard-earned and well-deserved commencement with an intimate ceremony in Sutardja Dai Hall’s Banatao Auditorium. Over 30 students from 20 different majors had classes and practice experiences upended by the pandemic, Prof. Clare Talwalker reminded the graduates and their families, all while war, oppression, and suffering did not abate.
“As champions of social justice,” added Prof. Dan Fletcher, Blum Center faculty director, “they represent the best of UC Berkeley.”
The curveballs thrown by the pandemic, however, did not compromise the intellectual rigor of the 17th GPP class’ courses of study.
“The classes were not prescribing a way to achieve social and economic equality. I wasn’t given a linear path where I could work my way up the ladder like some corporate job,” said Alisha Dalvi, a student commencement speaker and political science major. “Rather, GPP classes encouraged us to narrow in on ourselves and our community. I first had to come to terms with my engagement in systemic inequality before I jumped to finding a solution.”
Alisha Dalvi (Photo by Amy Sullivan)
Dalvi did her practice experience in Mumbai, doing research to identify the pros and cons of Indian government programs meant to assist farmers with sustainable agriculture practices. For her, GPP also fostered a vibrant community.
“The students in the minor are a very specific Berkeley niche,” she told her peers. “Meeting someone who is also a GPP student is like meeting a long-lost best friend. You’re guaranteed to discuss how fantastic the classes are, followed up by a complex conversation of structures of power.”
For Quiona Zamara Trimmell, the afternoon’s other student commencement speaker, the minor became a lesson in individual and communal commitment. The anthropology major, GPP peer advisor, and soon-to-be University of Sussex master’s student reflected on how the “mosh pit” of experiences we have throughout our lives as well as the values passed on to us lead us to our commitments.
Quiona Trimmell (Photo by Amy Sullivan)
“My hope,” she said, “is that this will foster a sense of humility in us, a sense of gratitude for all those, whether stranger or friend or somewhere in between, that fueled our sense of commitment to that which we have chosen to stand for” — namely, the long, slow, hard work of effecting change, rooted in community. “The commitment seems all the stronger when we know each other, when we can be held accountable, when we eat together, when we laugh and cry together, and when we care and love for one another,” Trimmell said.
GPP alumnus Christian Guerrero gave the keynote address. The Class of 2019 graduate — an arts and media activist, podcaster, and coffee importer — worked with the People’s Solidarity and Education Tours in the Philippines as his practice experience and now works at Tides Network, a nonprofit philanthropy organization.
The work students have already done during college is valuable in and of itself, he said, and should be recognized and spoken for by students as such. “Learn to advocate for yourselves so you can be in a position to serve others,” Guerrero said. “And connected to that is to acknowledge your own position and privilege and play your part” accordingly.
Christian Guerrero (Photo by Amy Sullivan)
Learn the language of power, he added, so that you can write your own story and a new story for your communities: “The more fluent you are in the language of power, the more you’ll see the opportunities to shift that power and create the impact you want to see.”
Echoing Trimmell, Guerrero pointed out that this crucial, often heavy social justice work is made all the more bearable by the support provided by the graduates’ families, friends, and communities — relationships they should hold fast to. And this critical work, and the perspectives the Class of 2024 brings, do not need others’ permission.
“Y’all, as graduates, have more than enough knowledge and are well equipped to take on the world,” Guerrero said. “I don’t like it when people say, ‘Wait until you get into the real world’ to students — very paternalistic, right?”
“It should be the other way around: The world is waiting for y’all to contribute, to give your own knowledge, to take these learnings and apply it out there. We need y’all.”
Soliver Ché Fusi is an environmental engineering PhD candidate at UC Berkeley. She hurries online to speak with me late in the Kenyan evening about her work at the Blum Center for Developing Economies. She’s telling me how the technology she’s working on hits on all these target issues — and it’s simple: sustainable agricultural fertilizer.
As we step into this first year of the United Nations’ International Decade of Sciences for Sustainable Development, the world still circles around the issue of global poverty. By one estimate, from 1990 to 2015, extreme global poverty fell from affecting over one third of the world population to only one tenth, decreasing about 1 percent annually. With the COVID-19 pandemic, it picked back up: from 2020 to 2022, each year pushed 1 percent back into poverty.
As progress reverses at the same pace it was made, with this Decade comes new urgency. How do the growing global poor access clean drinking water? How do we protect public health and food security with affordable, low-pollution food sources? How do we curtail the impacts of climate change on the global economy while centering carbon-lowering initiatives? Sustainability is critical; technologies must take away from carbon emissions, the consequences of which disproportionately affect impoverished communities. With so many moving targets, how does one choose which issue to aim for and check all those boxes? And who will do it?
Soliver Ché Fusi is an environmental engineering PhD candidate at UC Berkeley. She hurries online to speak with me late in the Kenyan evening about her work at the Blum Center for Developing Economies. She’s telling me how the technology she’s working on hits on all these target issues — and it’s simple: sustainable agricultural fertilizer.
“If you break down all the complications and nuances, I would argue that we just want clean water…healthy, nutritious, adequate food, and clean air,” says Fusi. But how does fertilizer do this? She explains: It diverts the human waste stream. Fecal and organic matter are collected and burned down to biochar, then mixed with undiluted urine. Nutrients in urine, especially nitrogen, are recovered. This becomes a sustainable amendment that, when applied to crops, returns nutrients to soil.
Fusi adds that it keeps pathogens from drinking water — and more. “If we’re recovering nitrogen from urine…that’s preventing degradation of water bodies,” she says. So, good for wildlife as well. This cheap fertilizer would also save — and make — money compared to current sanitation systems, and be affordable to low-income smallholders. Their livelihoods would also be improved: soil pH, microbial health, organic matter, and (of course) soil fertility mean better crops and better food security. Soil carbon is also sequestered — good for emissions.
Fusi is just one of many students, alumni, and faculty leading projects like this through the Blum Center, a nearly 20-year-old institution dedicated to combating poverty near and far via technological and policy innovation. Many disciplines come together here, most notably Development Engineering. Berkeley, the Blum Center, and its affiliated faculty can be credited for establishing this field, which combines engineering with other disciplines like human-centered design, resource management, social sciences, and business management.
Fusi’s work shows the Blum Center is — no pun intended — fertile ground for sustainability-minded academics and on-the-ground practitioners eager to make global social impacts. And not just through research: but through actualizing technological solutions to global poverty. It’s a crucible of possibility for those pursuing careers, higher academia, and entrepreneurship that could meet global demands for lowering carbon, while simultaneously improving quality of life in under-resourced areas. Other programs at the Blum Center overlap with the Development Engineering master’s program and PhD minor, including the Global Poverty & Practice (GPP) minor, the Big Ideas Contest, and the Health Tech CoLab.
Without these resources Fusi feels she wouldn’t be where she is now: Kenya, by way of California, seeing this project’s real-life results. “The Blum Center…was really the gateway into implementing the work,” she says. “Both times that I’ve been to Kenya, they funded the travel, which is not a small thing. … To do work, you have to be situated in that context. [The Center is] going to put money into that.”
Fusi is not even from California, nor from Kenya: She’s from Cameroon. Another facet of the Center is its “melting pot” nature. U.S. and international students mingle and collaborate closely; so do undergrads, graduate students, PhD candidates, post-doc academics, and faculty. The Center itself suggests that, to find solutions to global poverty, we’ll need an equally global-diverse group to cross-pollinate within itself. This attracts many ambitious students from abroad to Berkeley — including Yicheng Wei, another international student from Xi’an, China and recent alum of the Master of Development Engineering program.
Wei works a different angle on global poverty at the Blum Center: epidemiology, targeting the COVID-19 pandemic. With her cohort, she studies ways to test wastewater for anticipating where the virus spreads through low-income communities, which often don’t have accessible testing sites. “It’s changed me a lot…especially my personality,” she says of the Blum Center’s international setting. “I had a lot of ideas, but didn’t know where to show them. … I’m also more willing to share my own opinions.”
Wei is now applying for a bioengineering-focused PhD, with an offer already from the University of Tokyo. That said, Wei has also felt very challenged by fellow academics and faculty here — though in a good way. “The rest of the team are all PhD, post-docs, and scientists,” she says. “They have much more experience compared to myself, but they’re not like, ‘Oh, you know nothing!’” One of these experts is civil & environmental engineering Prof. Kara Nelson, the Blum Chancellor’s Chair in Development Engineering. Nelson is faculty lead for Wei’s project, and Fusi’s fertilizer project as well. “Professor Kara Nelson…guided us to a correct pathway,” says Wei. “She’s really passionate about every question I have.”
In fact, many Blum Center projects come under the purview of Nelson, who’s been at Berkeley for 22 years. Her academic focus has long been on water — but especially wastewater and the human waste stream. It greatly streamlines the whole water issue, she claims. “What always motivated me, since the beginning of my career, is how we can bring more attention and creative solutions to addressing this waste issue,” Nelson says. “Adequate sanitation is necessary to address so many issues that are linked — improving children’s health, protecting the environment, increasing food security, and creating respectable job opportunities. Also, if we aren’t adequately managing our waste, then we aren’t addressing one of the biggest threats to safe drinking water.”
Besides water there are other issues — Evan Patrick and Lambert Lin, two other Blum Center students, focus on forest restoration in low-income countries for capturing atmospheric carbon. Without the Blum Center’s international backdrop, it’s possible these two would have never met or worked together. Patrick — a PhD candidate in Environmental Science, Policy, & Management — is from the United States. Lin hails from Beijing, a recent graduate of the Master of Development Engineering.
Patrick, Lin, and others on their team take reforestation approaches a step further than most: assessing how impactful plantings really are. While carbon programs may help offset climate impacts on vulnerable communities, they claim they must also be feasible, fair, and transparent to the smallholder landowners actually doing them — and more incentivizing. To achieve this, their work focuses heavily on remote sensing, data collection, and predictive “forest models” to improve these initiatives while “de-privatizing” the data, making it more openly accessible and affordable.
It’s not easy — like Wei, Lin says faculty readily challenge their ideas. Says Lin of one faculty member, “He actually criticized the projects. … It helped us to fine-tune our conclusion.” Because of the possibility of policymakers using their work as an excuse to cut down natural forests, Lin and team were able to develop clearer and more airtight conclusions.
Lin’s and Patrick’s project faculty advisor, Prof. Matthew D. Potts, may have had a role leading them to think differently. Potts first established and funded this project at Berkeley. Referring to Patrick’s and Lin’s work, he says that it’s the data collection itself that allows for these kinds of projects’ impact assessments. “How do you assess the impact that motivates people to act,” he asked, “but also helps you design a better program?
Similarly, other faculty — like Nelson — pivot students away from the obvious towards issues people might not want to touch. “How we manage our waste is something a lot of people aren’t as interested in, or as comfortable talking about,” she says about focusing on the waste stream versus water alone. “It’s not, like, everyone’s favorite topic of conversation.”
That said, students also feel they get to challenge how things are done, both inside and outside the classroom. Patrick brought his own criticisms of reforestation work. “Some of the re-plantings…are like little pine matchsticks. … It feels like they kind of only do it one way,” he says. “I think that a lot of tree planting programs have huge trust issues globally. Having a larger data-driven approach to actually show what is working, and what is not — because there are good examples going on.” Lin concurs: “Planting trees is not the best way to sequester carbon. But there are co-benefits. … It could improve water quality, and bring less buildup of nitrogen, improve biodiversity, and improve soil erosion problems.”
Fusi feels the same about academia in general, where disciplines can be siloed and the technology can overshadow the human context. “We are told that research has to be done in a certain way to be considered ‘real science’” — as if it were a politically neutral endeavor, she says. “I think I would have conformed into what mainstream academia says is appropriate.” But her colleagues at the Blum Center with similar backgrounds to hers inspired her. Her cohort “was always like, ‘This is not okay. These things don’t have to be this way.’”
While innovation and interdisciplinary thinking are important, so is scalability. For some this means narrowing one’s focus to the obvious for quicker results — like clean water, pure and simple. Jeremy Lowe, a PhD student in environmental engineering with a Development Engineering emphasis, helms a passive-chlorination water project through the Blum Center and the Pickering Lab that provides low-maintenance, affordable, and electricity-free chlorination that disinfects drinking water, and that any developing country could access.
It could also be brought to scale, and rapidly. “Two-point-three billion people use a water drinking source right now that could potentially be compatible with this technology,” Lowe says, referencing a study. But he is also realistic. “This is not going to be the end-all-be-all solution for water treatment,” he adds. “Chlorination is doing a great job at disinfecting pathogens from the water, but it doesn’t disinfect all pathogens effectively. And it doesn’t address chemical contaminants. This is where combining chlorination with other water treatment methods is helpful.”
For some Blum Center academics, taking aim at global poverty issues comes from a personal place — bringing solutions to problems they witnessed growing up. Says Lowe, “I grew up in rural North Carolina, and I grew up fairly poor. I think that ultimately shaped how I perceive the world, and how I interact with it. … There’s a lot of unneeded suffering caused by global poverty.”
For Fusi it’s personal too, tied to Cameroon and her home. “My aunt is restarting the farm she had lost because of the war,” she says. “All this knowledge I can use, in a more career sense…but it can also go back to the people that are closest to me, and not just family.”
The diverse figures at the Blum Center bring different criticisms, talents, and angles to global poverty issues that urgently need new perspectives. They come from all around a globe hurtling into the International Decade of Sciences for Sustainable Development.
Besides the Blum Center as their home, something else seems to unite many of these voices: a desire to serve. “My ultimate goal is to be of service to people,” says Lowe.
“I consider myself a servant,” Fusi adds. “Determining who I want to serve, and how I want to serve them.”
Under a new NSF-funded research program housed at the Blum Center, the Digital Transformation of Development (DToD) Traineeship, students are using their research skills to apply digital tools, such as machine learning and AI, to the issues and challenges of poverty alleviation, disaster relief, and more — in pursuit of digital and technological justice, equity, and empowerment.
Navigating around town, tailoring our workouts to our level of physical fitness, knowing when our packages will arrive: The boom in data collection and analysis has been a boon to our daily lives — and a new paradigm for businesses, organizations, and governments to optimize efficiency and improve services. It feels ubiquitous. Who hasn’t taken advantage of the digital revolution?
It turns out, many communities haven’t been able to. From marginalized neighborhoods nearby to many areas around the globe, the tools that increasingly govern and improve our lives are not available or not tailored to serving everyone, be it personal wellbeing, environmental health, or economic security.
But under a new NSF-funded research program housed at the Blum Center, the Digital Transformation of Development (DToD) Traineeship, students are using their research skills to apply digital tools, such as machine learning and AI, to the issues and challenges of poverty alleviation, disaster relief, and more — in pursuit of digital and technological justice, equity, and empowerment.
“There’s a lot of recognition of the potential of rapidly emerging technologies like AI, new analytics, scalable cloud computing, and novel data sources,” says Matt Podolsky, DToD program coordinator. “But these advancements have not been particularly targeted to under-resourced communities and issues that pertain to them. We aim to address that shortfall.”
After an initial planning year, the five-year program kicked off Fall 2022 with its first cohort of nine master’s and 16 PhD students. Though their formal traineeships center around three DToD-themed courses that are taken over two or more semesters, the program aims to keep them involved for the entire duration of their graduate studies. A handful of fellows receive one-year awards covering tuition and fees, plus a stipend; the fellowship also offers the unique opportunity to apply for travel grants for self-arranged internships, where they conduct fieldwork and applied research with and within low-resourced communities. For PhD students, the program additionally allows them to work toward the designated emphasis in Development Engineering, an official minor for PhDs. The interdisciplinary skills developed in DToD include everything from technical writing skills to ethical data collection, all with the goal of producing fair and inclusive analysis to benefit underserved communities.
One of the key courses students take in the Development Engineering ecosystem, “Design, Evaluate, and Scale Development Technologies,” provides a hands-on opportunity to develop a tangible solution — say, a simple-to-use, easy-to-carry solar-powered water pump — to real-world problems — say, climate-impacted farmlands. The focus is always on incorporating the context and needs of people and their communities.
“It encourages students to develop a solution that involves the end users in the design process and could be scaled beyond just a small research prototype,” says Podolsky.
Another class, “DToD Research & Practice,” is a seminar featuring guest speakers including thought leaders and researchers from UC Berkeley’s faculty and experts in industry applying AI and data technologies for social impact, who work on everything from how to incorporate AI in development to finding early signs of eye disease using machine learning. This class also allows students to present their own work to peers, providing feedback to each other while learning about interesting research across campus. That model fosters collaboration, support, and skills in communicating research to those outside one’s discipline.
—
Rajiv Shah, former administrator of USAID and former Blum Center trustee, approached Prof. Shankar Sastry during multiple board-of-trustee meetings about building on the Center’s mission.
“The brand of the Blum Center is really technology and mechanisms, incentive designs, and so on to lift people out of poverty,” says Sastry, the Center’s former faculty director, the College of Engineering’s former dean, and DToD’s principal investigator. “And Raj said, ‘Why don’t you take it to the extreme? And why don’t you see how you can combine these latest greatest technologies?’”
Thanks to Development Engineering pioneer Prof. Alice Agogino, the Blum Center already had a track record of success with National Science Foundation Research Traineeship (NRT) programs. Meanwhile, Dr. Yael Perez, director of the Center’s Development Engineering programs and the coordinator for the InFEWS NRT, felt it would be a boon for students with digitally minded social-impact projects to receive the same kind of holistic support that InFEWS students had for their own social impact work. She hoped to see more social impact–minded students come out of programs like those of Electrical Engineering and Computer Science. And Shah’s idea came back to Sastry.
“It became rapidly clear that technologies in AI and machine learning, as well as Internet of Things and cloud computing, all of that was booming,” he says. But what he found missing was “how you would bundle them into services that could then be offered for people to better themselves, and at scale.”
Around 2019 and 2020, “by the time we were putting this [program] together, most corporate boardrooms were talking about digital transformation. And they didn’t exactly know what they were talking about,” Sastry adds. “But we taught that by digital transformation, we really meant: How do you take these advances in AI, machine learning, IoT, cloud and edge computing to provide services — be they in healthcare, in energy, in distributed energy management — to be able to really enable economic development.”
“We could give our students an appreciation not only for these algorithms,” he says, “but also what happens when you use them.”
—
The first cohort’s fellows come from disciplines and departments across campus, from various branches of engineering to city and regional planning to the School of Information. Over 60 percent of the first cohort are women and nearly half are underrepresented minorities.
Ritwik Gupta works with collaborators at the United States Geological Survey to measure soil water retention after the 2021 Dixie Fire. (Photo by Matt Podolsky)
Among this first class is Ritwik Gupta, a PhD student at Berkeley’s AI Research Lab, who focuses on computer vision for humanitarian assistance and disaster response, along with public policy for the effective and safe usage of such technology. Working with a diverse set of partners such as CAL FIRE, the Department of Defense’s Defense Innovation Unit, and the United Nations, his research on tasks such as assessing damage to buildings from space and detecting illegal fishing vessels in all weather conditions has been deployed worldwide.
The work of classmate Evan Patrick leverages geospatial science and ethnography to evaluate forest restoration efforts in Guatemala and explore the ongoing impacts of the El Niño Southern Oscillation on landscapes and livelihoods in the country. The Environmental Science, Policy, and Management (ESPM) PhD student worked with two MDevEng capstone groups in the Potts Lab to model the carbon benefits of plantation expansion in Guatemala and to use social media audience estimates to investigate ENSO-driven internal migration in Central America.
Sarah Hartman, in her fifth year of an ESPM PhD program, first got involved with the Blum Center through its first NRT on innovations in food, energy, and water systems. She wanted to continue what had been an “absolutely wonderful experience,” and DToD just happened to be relevant to her work using technology, engineering, and science to improve water and agricultural conditions in low-resource settings.
“The way the program’s designed is really nice,” she says, “because it gives you exposure to people who might be outside of your discipline but are using methods that might be of use to your particular application.” For instance, in one DToD class, a visiting professor discussed how she translated the skills and technology involved in using AI to build others’ personal wealth into using AI to detect early health concerns in low-resource settings.
The programs’ benefits, however, extend beyond official class content.
“I really appreciate the balance they strike between professional opportunities and community-building opportunities,” Hartman says. “And sometimes it’s the small things.”
Ritwik Gupta points to dark vessel detections generated from his xView3 AI model within the Department of Navy’s SeaVision platform. (Photo by Matt Podolsky)
Like coffee and cookie breaks. Students like Hartman find inspiration and collaboration during opportunities to socialize during class. “There’s a lot of value in the informal conversations that we have around the structured lecture content,” she says.
Take, for instance, Gupta’s work using machine learning and satellite imagery to understand the toll Russia’s war in Ukraine is having in cities. His methods, Hartman found, could add a new layer to her work understanding how the war is impacting Ukrainian agricultural resilience, such as better, faster insight into the status of key agricultural infrastructure like grain silos and ports. This cross pollination improves her ability to conduct real-time analysis in a continuously evolving situation.
—
Going forward, Podolsky plans to implement more workshops on topics from data visualization to effective communication skills, such as op-ed writing. “We really just want to add to the research training aspect beyond just coursework,” he says.
But in the big picture, Sastry says, the DToD program is about more than just the implementation of digital development solutions in accordance with the needs of people in under-resourced settings. It’s also about what comes before that process even starts.
“I think it’s great to do interventions, it’s great to think about clean water, it’s great to think about energy,” he says. “But what’s really emerging from this series is students getting a sense of empowerment to go and change the world. And that quite often transcends specific solutions. I think we’re giving them that, and we’re giving them some optimism.”
“Because at the end of the day, the technology is great, but it’s the starting point,” he adds. “It’s not the endpoint; the services are the middle point; and then the empowerment for people is really the endpoint. So it starts with empowering our students to empower the people to help themselves.”
“FireTools,” developed in DevEng C200, “Design, Evaluate, and Scale Development Technologies,” brings a wide array of resources under one umbrella for local decision-makers to use to improve disaster preparedness, response, recovery, and resilience — with a particular emphasis on doubly vulnerable communities.
In California, it’s hard to overstate the impact of climate change–fueled wildfires: Over the last few decades, we’ve seen a 320-percent increase in burned areas, 268 lives lost, and in just the past five years, an estimated $60 billion in lost revenue.
At the national level, the US Department of Housing and Urban Development is also concerned about wildfires as it focuses on post-disaster recovery, and there exist a variety of wildfire-resilience toolkits meant to guide decision-makers’ efforts to help people prepare for and recover from wildfires. But according to Erica Anjum, there is not enough attention on low-resource areas. These communities are doubly vulnerable: not just at greater physical risk from wildfire but also facing “intersectional social vulnerabilities,” says Anjum, a city and regional planning graduate student. Indicators of these can include, but aren’t limited to, income, housing status, age, and disabilities. “Different vulnerabilities render people vulnerable in different ways — all of which are relevant in planning resilient communities,” she says.
Enter “FireTools,” an online toolkit prototyped by Anjum and her graduate-student teammates in DevEng C200, “Design, Evaluate, and Scale Development Technologies.” Their toolkit brings a wide array of resources under one umbrella for local decision-makers to use to improve disaster preparedness, response, recovery, and resilience — with a particular emphasis on doubly vulnerable communities.
FireTools is a hub for resources such as community- and fire-mapping tools, funding sources, landscaping best practices, evacuation preparedness and resilience centers, and data-privacy considerations — all things decision makers rely on when assisting and preparing communities before, during, and after catastrophes.
“Apart from the very crucial impact on loss of lives and property, the intervention will lead to more collaboration between stakeholders in the fire preparedness, resilience, and recovery spaces,” said Master of Development Engineering student Titli Thind. “The process of building the toolkit has spurred conversation between previously disconnected key decision makers, and we hope that this continues.”
DevEng C200, a core MDevEng course open to grad students from a variety of backgrounds, provides an opportunity for students to partner with professionals to tackle problems that require the skills of Development Engineers. That process requires understanding the focus area’s stakeholders, end users, and their contexts; testing hypotheses for effective technological intervention; iterating these solutions’ designs; evaluating their efficacy; and proposing a way for scaling up their use.
Professors Amy Pickering and Mathieu Aguesse lead the class. Class projects have included an app for farmers to engage with one another, build community, and monitor the health of their wetlands; a comprehensive handbook for more efficient greenhouses for farmers in the climate change–impacted eastern Himalayas; expanding and diversifying the products and market for plastic-recycling social enterprise Takataka Plastics; a mobile platform, focused on data-governance management, that allows for the collection, sharing, and analysis of data from low-resource settings; analyzing and modeling the widespread deployment of a water-chlorination device; a simple-to-use, easy-to-carry solar-powered water pump; an affordable, foaming soap dispenser; improving the outcomes of unhoused people with a better online platform that’s used by both unhoused folks and San Francisco caseworkers; and the improved integration of frontline public health workers in a platform that provides primary-care services in Guinea.
Along with Thind and Anjum, FireTools was developed by Xuan Huang (MDevEng), Kanyawee Srikulwong (development practice), and Ashley Woodward (civil and environmental engineering).
The team started with research data on wildfire resilience, practices from other fire-prone regions like Australia, and 14 case studies of communities and their decision makers who have faced fires before. They spoke with first responders and planners from previously hard-hit California communities. Their due diligence brought to light specific problems that the team sought to address, such as multiple authorities or organizations collecting the same data in the same communities post-fire (which risks retraumatizing vulnerable fire survivors) as well as some neighborhoods’ lack of accessible evacuation routes.
“This project is a great example of how valuable it was to interact with the wildfire toolkit’s end users to create a product that addresses their needs,” Pickering said.
The tools in the kit — such as a post-fire data-collection process and landscaping best practices — evolved and grew with further stakeholder interviews and feedback, culminating in the website, a toolkit distribution plan, and a business model. The plan is to provide the toolkit to primarily local decision-makers and planners for free, with the team proposing funding for growing, improving, and testing it from primarily federal agencies with a stake in disaster-resilient communities.
The team built its toolkit as a “living document,” where the at-risk communities themselves can share their own insights and experiences to further refine authorities’ ability to help them. Those same authorities can use the toolkit to further inform their disaster planning and coordinate with other agencies with whom they’ve historically had limited collaboration.
This whole process of producing a technological intervention in accordance with end users’ needs, however, is not over once the toolkit is put to use; it won’t be much good if it’s not sufficiently achieving its goals.
So, the team plans to measure their solution’s efficacy by, among other standards, the number of planners who take up the toolkit, collecting feedback from decision-makers in places hit by wildfires, examining whether its use has streamlined data collection, and whether doubly vulnerable populations’ trauma associated with collecting sensitive data after a catastrophe — worsened by duplicative surveying — has been reduced.
Researchers from UC Berkeley, UCLA, and UC Merced will continue working on the toolkit, Anjum says. But regardless of how the toolkit may have to be adapted, its goals continue to be reduced loss of life and property, improved data collection and interagency dialogue, and all-around better wildfire preparedness and resilience.
“We want to share our experiences and expertise,” one local planner and survivor of the record-breakingly deadly and destructive 2018 Camp Fire had told the team, “so others don’t lose as much as we did.”
SHE uses sustainable fashion design to empower talented rural women to break free from generational cycles of poverty while promoting rich African heritages to the world. The project helps women with years of skilled seamstressing experience who find themselves disregarded or deemed incapable due to the rural environment and a male-dominated society.
In the summer of 2021, Patricia Quaye took a 15-hour journey from her home in Awutu Breku, a small town in Ghana, to Berkeley to be a part of the inaugural cohort of the Master of Development of Engineering program, housed at the Blum Center for Developing Economies. While she was 7,000 miles away, her heart remained close to home, and in the summer of 2022, Quaye went back to Ghana to build on her organization dedicated to giving back a better livelihood to her community.
Quaye had founded SHE 4 Change in January of that year as both a business and a foundation to provide women in her community with more opportunity; SHE stands for Support Her Empowerment. “That is exactly what the project is doing,” says Quaye.
Patricia Quaye wears SHE 4 Change, featuring traditional African prints. (Courtesy photo)
SHE uses sustainable fashion design to empower talented rural women to break free from generational cycles of poverty while promoting rich African heritages to the world. The project helps women with years of skilled seamstressing experience who find themselves disregarded or deemed incapable due to the rural environment and a male-dominated society. These women are often paid much less than what the cost of materials and their labor are worth. SHE aims to break this cycle of poverty by paying women fairly and expanding their market. Quaye took advantage of her time as a student in Berkeley to study the global market and adjust her designs to a broader range of individual tastes while sending the profits back to women in her community. The high quality of SHE apparel extends its customer base beyond those who can only afford the simplest clothing.
Quaye recalls, from her conversations with the seamstresses, instances prior to founding SHE 4 Change where customers didn’t return to pick up their clothes after dropping them off for sewing, as they, too, were poor and may have later decided they could not afford the sewing costs after all. Some even refused to pay the previously agreed-upon cost. This leaves many women stranded.
“Imagine going through four-plus years of training to acquire a skill, but because you are located in the ‘wrong’ place and people don’t know about your skill, you don’t grow professionally, and you can barely put food on the table,” Quaye says.
Quaye’s cousin, a seamstress for over 15 years, inspired SHE 4 Change. When COVID-19 hit, Quaye saw her struggle — her cousin lost her few and only patrons to the pandemic, leaving her unable to afford even a basic meal. Quaye wanted to help and began looking for organizations that could assist skilled women like her cousin find patrons or obtain resources. But she couldn’t find any support, with many organizations unresponsive or simply declining to help. Quaye wanted to take matters into her own hands.
A SHE seamstress sews with her own machine at her own home. The social enterprise plans to hire many more seamstresses before officially launching in the spring. (Courtesy photo)
Quaye’s project-based classwork in the MDevEng program required her to connect more deeply to the community she’s serving. After conducting research and interviewing women, she realized this was a challenge across many regions and communities in Ghana, not just for her cousin. Rural women often lack the tools to sew high-quality garments, therefore most individuals living in big cities and urban areas, who can afford higher quality wares, don’t “believe” in rural women’s capacity to produce the quality they require, she says. This limits seamstresses to rural markets with lower rates for their work hours.
Quaye cites her own experience for her dedication to creating opportunities to break the cycle of poverty. “I grew up in a poor background,” she says. “I know what it means to not have opportunity. I know what it means to not have food on the table or know when the next meal you’re going to eat will be.”
The SHE 4 Change logo holds cultural significance in and of itself: The “E” is a tribal Ghanaian symbol signifying sankofa. (Courtesy photo)
So over the summer of 2022, along with a summer job and internship, Quaye went back home to her small town of Awutu Breku to be hands-on with her fashion enterprise. This entailed working with her mother to create designs, searching for and purchasing fabric in Accra, Ghana’s capital, from female vendors, and bringing fabric and supplies back to the seamstresses who then sewed the designs using their own machines. While SHE seamstresses can repair existing clothing, they focus on making new ones from scratch, supporting women fabric vendors as well. These fabrics are traditional African prints and patterns which hold historical and cultural significance. The SHE logo itself showcases the traditional Ghanaian symbol of the sankofa in the “E,” a bird that signifies retrieving good from the past.
The most valuable part of her time at home, however, was the face-to-face interaction she had with her team — getting to know the women in person rather than over the phone. She had met these seamstresses through her mother, a community organizer who encourages girls to get involved in political decisions that affect them. Her mother provided Quaye with connections and further instilled the importance of empowering the women around her. Quaye shared the excitement of the project with them, learned the impact it could have on them and their families, and came to better understand her seamstresses’ work environment.
A pile of fabrics sourced from vendors in Accra, the capital of Ghana. Quaye typically finds her fabrics at larger markets in the city and brings them back to Awutu Beraku. (Photo by Patricia Quaye)
Nowadays, SHE’s piloting stage features six women, but Quaye plans to hire over a dozen more before an official launch. She officially registered SHE 4 Change as a company and a foundation, obtained a company bank account, and created social media accounts for the brand.
More challenging are the finances. Quaye had used her Berkeley scholarship stipend to cover fabric, packaging, and other production costs. But she also went looking for funding from both NGO- and government-sponsored, women-oriented organizations to provide her seamstresses with reliable machinery to guarantee a better and safer working environment. As more profit comes in from an international customer base, equipment can be purchased to lower the seamstresses’ time and effort, thereby lowering the cost of labor. This then allows for their service to be affordable for their own community as well, creating a chain reaction of relieving financial insecurity. And as the foundation grows, Quaye hopes to train more women. “It’s important that this project allows women to empower themselves, so they can empower other women as well,” she says.
Since graduating from the MDevEng program, Quaye has continued gaining experience as the sustainability coordinator at a retail company in the Bay Area, where she’s deepened her understanding of the clothing industry. In
Members of the MDevEng community sport SHE 4 Change clothing. (Courtesy photo)
July 2023, Quaye was awarded with the Mastercard Foundation Alumni Scholars Impact Fund, powered by the Big Ideas Contest. With this funding, she is building a SHE 4 Change Sewing Center in Awutu Breku, and in March will head back and officially launch the SHE 4 Change line of products. She hopes to get more funding through other channels to support the project. All the while, she continues monitoring the impact of education on women in Ghana and is committed to follow up with research that can expand the impact of SHE 4 Change and similar endeavors to more countries through the SHE 4 Change Foundation.
“I don’t want people to buy just to help the women, but because the women can produce quality products, and they feel the value when wearing the clothes,” she says.
Indeed, Berkeley peers and teachers who have tried SHE 4 Change’s wares have loved them and become patrons. “The support from the DevEng department, my classmates and professors, always pushes me to know I am making an impact. It is like a family that is on the same mission with me,” she says.
The MDevEng program itself has played a massive role in how she approaches her foundation, ensuring that she stays tuned to the needs and aspirations of the women on her team.
Going forward, Quaye hopes to see SHE 4 Change take off into a global brand known for empowering women while providing unique clothing. She also hopes to continue to break Eurocentric barriers by using fashion to showcase traditional African prints. Instead of having the world dig out culture and resources in Africa, she says, “we can bring the culture to the world by keeping heritage and local women alive through our garments.”
Yordanos Degu Zewdu’s journey to becoming a changemaker began as a child in Addis Ababa, inspired by a moment of compassion from her mother. At UC Berkeley’s Development Engineering graduation, she urged classmates to embrace resilience and unpredictability, fueling hope for a more just, equitable world.
Yordanos Degu Zewdu clearly remembers the moment she decided to become a changemaker helping those most in need: as a young kid in Addis Ababa, on the way home from shopping with her mother, right before the start of the school year.
Degu Zewdu and her mother came across a father and his two children. He appeared ill and was begging desperately for food for his hungry kids. The suffering and desperation moved the young Degu Zewdu deeply.
“But as a kid, I had no means to help. So I stood there, overwhelmed by a sense of helplessness,” she recalled. “My mother, the kindest person I’ve ever known, generously gave the father money to buy food for his kids, brightening their faces with joy.”
Yordanos Degu Zewdu (Photo by Amy Sullivan)
In that moment, she realized that “when I grew up, I wanted to be in a position to help communities and families in need.”
Degu Zewdu, who continues fulfilling that promise as a Development Engineer, recounted the story to her peers and their families last Friday evening at the commencement ceremony of the UC Berkeley Master of Development Engineering program’s Class of 2023 — the second-ever cohort of what is likely the world’s first such degree program. The group of 30, hailing from 13 countries, crossed the stage at Banatao Auditorium following three semesters, an internship, and a capstone project.
“We are here to celebrate the hard work you have put into this program and to honor your commitment, your courage, your tenacity, and your compassion,” said Prof. Kara Nelson, chair of the Graduate Group in Development Engineering. “And we thank you for the work that you are doing to make this world a more just place, a more equitable place, and more peaceful. You are an inspiration to all of us.”
The Class of 2023 worked on projects ranging from tracking and optimizing plastic waste collection for recycling in Uganda, to household sanitation and hygiene in Ethiopia, to policy needs as California transitions to greater renewable energy.
Despite impressive accomplishments in the classroom and out in the world, the variety and magnitude of the world’s problems can make DevEng work feel “like planting a singular seed in a vast desert and hoping for a forest to grow tomorrow,” said the evening’s other student speaker, Anjali Ravunniarath.
Anjali Ravunniarath (Photo by Amy Sullivan)
“I stand here, with the same big problems and no easy solutions. However, I have found solace in this community in the last year and a half,” she said. “Together, we’ve dissected a lot of systems, understood parts of it, and occasionally tried to see if we could fix a few. The problems may not have disappeared, but our collective efforts make it seem less daunting, and that’s truly what I’m grateful for.”
This constant change-making journey won’t always be smooth sailing, counseled the evening’s commencement speaker, Ranjiv Khush, a water scientist, member of Marin County’s water board, and co-founder of Aquaya, a nonprofit producing data and tools to support universal access to safe water, sanitation and hygiene. Even the most accomplished development engineers, like Prof. Amy Pickering, don’t get it right every time, he said.
“Here’s the thing: Amy and all of our other heroes, they make embarrassing professional mistakes. They mess things up. They feel ashamed,” he said. “Just like us.
Ranjiv Khush (Photo by Amy Sullivan)
“The difference,” Khush added, “is that they’re really good at rolling with it. They shake it off. They refuse to let their mistakes define them. Be the same: Shake it off. Please, do not let your mistakes and your embarrassments dissuade you from anything or get in the way of your success.”
Prof. Dan Fletcher closed out the ceremony with a challenge to the newly minted master’s-degree holders: “I want to challenge you each day after this program, as you move on with your careers, as you find your passions, as you live your passions, to be the best person that you imagined you could be while you were in this program.”
It was a sentiment with echoes of advice Degu Zewdu had offered earlier in the evening.
“As we set forth on our individual journeys,” she said, “I urge each of you to embrace life’s unpredictability, step out of your comfort zones, show resilience, remain open to the countless opportunities that await. It is in these moments of growth and uncertainty that we will unveil the authenticity of ourselves.”
DevEng Photo Contest Winners Highlight Both the Promise and Fragility of Technological Interventions
Development Engineering is a field of research and practice that combines the principles of engineering with economics, human-centered design, entrepreneurship, natural resources, and social science to create technological interventions in accordance with and for individuals living in low-resource settings. It’s a technical field, one often rendered in blueprints, lines of code, and physical devices.
But depicting DevEng to lay audiences is vital not just to raising the field’s academic profile but to growing the capacity of a discipline that tangibly improves lives as well as to highlight the richness and complexity of the communities DevEng aims to serve.
Each summer, students in UC Berkeley’s Master of Development Engineering program and the PhD designated emphasis in DevEng implement DevEng interventions close to home and far away, documenting their work and their environment as they go. This year’s DevEng Photography Contest highlights the best of this summer’s photos and videos, from the sometimes-precarious state of electrical power in rural places to novel technologies for delivering medicines and medical supplies. (Coincidentally, the three winners were captured in the same country.) Jacob Seigel Brielle and Isaac Seigel-Boettner, the talented Cal-alum duo behind Pedal Born Pictures, joined DevEng staff in judging this year’s submissions.
1st place
“The fragility of rural power”
Samuel Miles, PhD student, Energy & Resource Group; DevEng designated emphasis
“This is a picture of a young boy carrying out his chores in rural Rwanda,” says Miles. “The background shows rural infrastructure — in this case, a sagging power line held up by a local tree. It encapsulates the opportunities and challenges of modernity — the possibility that the boy grows up benefiting from electricity, but also the dangers poor planning represents to safety.”
Judges commended the great intersecting lines in the composition and how the photo’s symbolism deepens the more one dives into the image.
2nd place
“Zipline Drone Landing”
Rachel Dersch, Master of Development Engineering student
Dersch’s video depicts a medical delivery drone landing. The company behind it, Zipline, is a Silicon Valley start-up operating in various African countries, including Rwanda. “They make deliveries constantly to all the hospitals in Rwanda that contain blood, medicines, and supplies,” says Dersch. The company provides “quality employment” for their staff in Muhanga, Rwanda, she adds, and is being considered for her research team’s sites for solar power and water filtration units, since they require a landing pad for deliveries. “The drones are a really cool adaptation for developing countries when the road infrastructure makes time sensitive deliveries like blood difficult to accommodate,” Dersch says.
Judges appreciated the depiction of a fascinating new technology being used for good — and the importance in DevEng of testing tech first.
3rd place
“Rural health clinic energy transitions in Rwanda”
Rachel Dersch, Master of Development Engineering student
“I like this photo because it showcases the complexity of working in rural locations where cows are grazing on hospital grounds next to new technology implementations,” Dersch says. “This photo was taken in a very remote location in the ‘Thousand Hills’ of Rwanda, a gorgeous place. We were at the location conducting qualitative interviews on the energy transition at the health clinic and picking up power monitoring sensors.”
Judges recognized this photo for the deeper story and symbolism behind it. Plus, “these sorts of juxtapositions help explain more of the why behind DevEng,” Seigel Brielle says.
Water, sanitation, and hygiene are crucial pillars of public health initiatives and in the fight against poverty. Issues like inadequate water access and poor sanitation disproportionately affect under-resourced communities, leading to waterborne diseases and socioeconomic impacts within vulnerable populations. Solutions are interdisciplinary, blending research findings and policy interventions in pursuit of infrastructure development, with communities’ contexts and needs at the core of WASH efforts.
In 2007, the Blum Center hosted UC Berkeley’s first Water, Sanitation, and Hygiene (WASH) symposium for scholars and development practitioners. The event was the first of its kind in the Bay Area, and for the next decade, Stanford and Berkeley hosted WASH events on alternating years. After a hiatus due the pandemic, the symposium was back this year for the first time since 2019. This time, it’s the Blum Center continuing the tradition, with a wider scope of research and a larger community since the original WASH event over 15 years ago.
Water, sanitation, and hygiene are crucial pillars of public health initiatives and in the fight against poverty. Issues like inadequate water access and poor sanitation disproportionately affect under-resourced communities, leading to waterborne diseases and socioeconomic impacts within vulnerable populations. Solutions are interdisciplinary, blending research findings and policy interventions in pursuit of infrastructure development, with communities’ contexts and needs at the core of WASH efforts. Practitioners range from chemical and environmental engineers to public health professionals.
On December 6, the Blum Center hosted graduate students, professors, and experts with one common connection — a commitment to sharing and expanding collective knowledge in the WASH sector. The event kicked off with an introduction from its head coordinators, Prof. Amy Pickering, Blum Center Distinguished Chair in Global Poverty and Practice, and Prof. Kara Nelson, Blum Chancellor’s Chair in Development Engineering. Icebreakers followed, where attendees broke out into teams to play a sanitation-inspired game.
The main attractions, however, were six longer research presentations and 17 quicker lightning talks, which included research developments that have concluded, are currently underway, or still in planning stages. They covered biological, environmental, and social issues, from cost assessments of water supplies to chlorination techniques for reducing maternal and neonatal diseases to proposing a compostable toilet.
The sheer scope of presentations demonstrated the multifaceted range of the field. “WASH challenges primarily affect low-resourced and underserved communities,” says Nelson. “Those in the field have to understand these problems from an interdisciplinary perspective.”
J’anna-Mare Lue, a Berkeley PhD student, was awarded a golden toilet trophy for the “Most Creative” presentation. Her lightning talk emphasized the social and environmental equity aspect of WASH work. (Photo by Hannah Wharton)
The end of the night featured a reception and awards. Joyce Kisiangani, a UC Berkeley PhD student, won for Best Visuals for her presentation introducing a low-cost passive-chlorination device for disinfecting water at the point of collection. Another UC Berkeley PhD student, J’Anna-Mare Lue, won for Most Creative for her presentation on water as a medium to address environmental inequity. Christine Pu, a PhD candidate at Stanford, was awarded Most Engaging for her discussion of how investments in water infrastructure transform rural livelihoods in Ethiopia.
The event was deliberately small and intimate, designed to cultivate in-depth conversations and small-group discussions. “It is an event by and for the people who participate in the WASH field,” Nelson says. Hannah Wharton, a environmental engineering PhD student in Pickering’s lab and a member of the WASH symposium student committee, agreed. “Connecting with other researchers and professionals in the WASH field is so important for making progress on the global inequities that we are all trying to eliminate,” she says. “Having people there from a variety of fields really speaks to the interdisciplinarity of WASH and the need for future events.”
A WASH attendee asks a question at the end of a research presentation. (Photo by Alisha Dalvi)
With around 60 attendees and plenty of time for networking, WASH aficionados were able to dive deep into the complexities of their peers’ projects. “Compared to the scale of the problems, we are a relatively small group of researchers working on them,” says Nelson. “We have to be resourceful and work in teams. And have a strong community that is supportive and lifts you up when you are feeling discouraged.”
When asked what they hoped to see in the future for WASH events, nearly every attendee had a similar answer: “To see more people!” They are certainly on track to meet this goal — each year, event planners have welcomed more and more first-time attendees. The increase in symposium attendance parallels new and expanding research projects in the field, like those of Kisiangani, Lue, and Pu. And as the WASH sector grows, these symposia are vital to encouraging collaboration and fostering a network where projects can succeed on an individual and community level.
“Next year,” Wharton says, “we want to host even more members of the community and continue increasing dialogue.”
Innovators@Cal — UC Berkeley’s annual flagship entrepreneurship event, which brought together aspiring student innovators, students curious about joining early-stage ventures, and an inspirational keynote speaker tackling the “world’s dumbest problem.”
Earlier this fall, UC Berkeley debuted a webpage spotlighting the breadth and depth of its most innovative alumni and the resources available on campus to support the next generation of game-changing entrepreneurs, along with a series of deep-dive stories highlighting Cal founders and their impacts on society.
The timing couldn’t have been better: Pitchbook recently ranked Berkeley No. 1 for number of venture-backed startup companies, ahead of the likes of Stanford, Harvard, Penn, and MIT. Berkeley innovators like Jennifer Doudna and Kevin Chou generate international headlines. Campus is home to an ever-growing number of entrepreneurship, innovation, and tech-minded organizations and resources.
But — for the aspiring student innovator with a rapidly germinating new idea — where do they start? Where can they access resources and support to help transform their ideas into reality? Where can they find teammates ready to go all-in?
On November 7, that place was Innovators@Cal — UC Berkeley’s annual flagship entrepreneurship event, which brought together aspiring student innovators, students curious about joining early-stage ventures, and an inspirational keynote speaker tackling the “world’s dumbest problem.”
Students from a wide range of disciplines and departments across the UC Berkeley campus took turns offering two-minute pitches to a standing room–only crowd in Banatao Auditorium. They highlighted a wide range of innovations, including an app detecting stroke symptoms, an electrical grid–monitoring technology, and simple new methods for improving the availability of menstrual products. Immediately after, speakers and listeners alike gathered in Blum Hall for a lively networking and brainstorming session where students used whiteboards to sketch out their ideas, solicit feedback, and find teammates.
Student entrepreneurs prepare for the evening’s networking session. (Sam Goldman photo)
One of those blueprints was for the startup Materri, which generates recommendations for the best materials to use in footwear designers’ products, saving those producers time and money in consulting fees. Materri attended Innovators@Cal hoping to recruit software engineers.
“We’re not software engineers, and we’re building a software platform,” said co-founder Kira Erickson. “So that’s been our main hurdle in becoming a successful startup: just finding engineering talent, so we’re hoping to find some talented people to work with us.”
Across the room was Kerisha Burke, who, after researching why Black people hold a disproportionately low percentage of STEM jobs, found that part of the problem was rooted in student opportunities. “Students from underrepresented backgrounds continue to face challenges in pursuing careers in the STEM industry,” she had told the audience, “particularly due to the lack of access to resources that could help them to succeed.” Many of these resources exist outside the classroom — STEM conferences key among them. But these events are expensive to attend and time-consuming to apply for.
MBA student Kerisha Burke pitches Scholarly Loop. (Sam Goldman photo)
Enter Burke’s Scholarly Loop, an AI-powered platform consolidating all manner of resources to support underrepresented students throughout the entire conference process, from a list of conferences to travel scholarships to tools that facilitate the paperwork side.
“I’ve been looking for an opportunity to pitch,” she said. “And I thought this was an opportunity for me to be vulnerable, open, and to just take a risk. Hopefully this is the first step in me doing that, then going out there and pitching and just getting more comfortable with sharing my ideas with others.”
The night’s guest of honor was keynote speaker Komal Ahmad, founder of Copia, a logistics technology platform for managing food waste. Ahmad, winner of the 2012 Big Ideas Contest, studied international health and global development as well as Global Poverty and Practice at UC Berkeley, before her work solving hunger earned her an avalanche of accolades, including landing on Forbes’ 30 Under 30 list. Copia redirects leftover food and meals (including from the Super Bowl and the Oscars) to organizations and people who need it now. The company has saved over 6.5 million tons of food, delivered over 5.4 million meals, generated over $21 million in savings for businesses and nonprofits, and operates in 40 states.
The story behind those eye-popping numbers is a single meal that an undergraduate Ahmad, then studying to be a doctor, hadn’t intended to have.
Komal Ahmad, founder of Copia (Sam Goldman photo)
Walking down Telegraph Avenue, she encountered a homeless man asking for food, and she invited him to join her for lunch. As he wolfed down his meal, he shared his story: His name was John and he had returned from his second tour in Iraq to find that his military benefits hadn’t kicked in. He hadn’t eaten in three days. And yet, “right across the street,” Ahmad said, “Berkeley’s dining hall was throwing away thousands of pounds of perfectly edible food.”
Hunger was not a problem of insufficient food, she realized, but a logistics and distribution problem.
“Solving the world’s dumbest problem became my life’s mission and Copia’s purpose,” she said. “Had I never reached out to that homeless veteran, had I never looked up from my phone, Copia would not exist. That day I fed one man. Because of his story, Copia will feed 8 million people” this year.
Yet the journey from one to 8 million was anything but linear.
Ahmad’s first attempt to find new stomachs for 500 leftover sandwiches on short notice had hardly any takers. Fast forward to subsequent efforts where she recruited her own volunteer drivers to ferry food from A to B, then tapped into the existing infrastructure of Doordash and Postmates to scale her endeavor. But after three years, Copia had yet to make much of a splash locally, and Ahmad felt depleted. “I lost my passion,” she said. “I lost my fire.”
She took a job at Google, listening to the complaints of angry customers for six months before getting fired. She had hit “rock bottom.”
But her dismissal was the “best thing that ever happened to me.” The intensity of failure, she told students, provides one with a new clarity, allows one’s strengths to shine through, and one’s “genuine self emerges.”
Ahmad returned to her passion, first volunteering at a Silicon Valley food pantry and then recruiting more volunteers. She built the technology and logistical systems to connect all manner of businesses and nonprofits so that leftover meals can find recipients who need them now. Copia joined the prestigious Y Combinator accelerator and became a multimillion-dollar startup.
“It’s not an overnight transformation,” she said. “It’s taking this step over and over — to take the risk, chase the dream, and follow your heart.”
“Whatever comes your way,” she advised, “keep moving forward.”
That, in a nutshell, is one of the key attributes of a successful entrepreneur, and a life view that UC Berkeley inspires, teaches, and supports. So remember to get your Big Ideas proposal in by December 6 — take a cue from Komal and take that risk. We are here to support you!
October 17 marked the International Day for the Eradication of Poverty, a UN observance to uplift the voices of those in poverty. Aligned with this mission, UC Berkeley’s Blum Center offers programs like the Global Poverty & Practice minor, Master of Development Engineering, Big Ideas Contest, and Health Tech CoLab, giving students hands-on experience in addressing poverty’s root causes globally.
Keerthi Konda, a senior cognitive science major, completed the practice experience of her Global Poverty & Practice minor over the summer, providing geriatric and palliative care to rural populations of India. As a pre-med student, Konda knew she wanted to tailor her experience to increasing access to healthcare. Each day she assisted doctors and nurses working in outpatient geriatric clinics, home visits, and hospice services, as well as conducted financial surveys with the families of patients for a new integrated facility to scale up its current services and reach more people from surrounding areas.“The GPP minor has changed how I view poverty and inequality. By combining theory and practical application, I’ve realized that poverty alleviation work is layered, with different approaches best suited for different communities, rather than one universally effective solution,” says Konda. “It’s about empowering communities and building a support system so individuals have access to basic needs, rather than just financial assistance.”
Keerthi Konda, a senior GPP student, is also a peer advisor for the program (Courtesy photo).
October 17 was the International Day for the Eradication of Poverty, a United Nations observance to acknowledge the efforts and struggles of those living in poverty and to uplift their voices to make their concerns heard. These goals are at the heart of the Blum Center’s mission, with academic, research, and extracurricular opportunities and initiatives encouraging students to consider poverty alleviation. The Center’s programs, including the Global Poverty & Practice minor, the Master of Development Engineering, Big Ideas Contest, and Health Tech CoLab, help undergrads and grad students find opportunities to get hands-on experience with alleviating the root causes and various manifestations of poverty locally and globally.
Blum Center students have launched a company that works with a women’s cooperative to grow and raise food in a 100-percent circular, sustainable system; started a company that turns otherwise-unrecycled plastic into usable household goods; evaluated the effectiveness of outsider-supported health-clinic microgrids; created a platform for unemployed recent graduates to develop and highlight their professional skills; and supported efforts to provide healthcare to those transitioning out of incarceration.
Excellence Anurika Joshua is a first-semester Master of Developing Engineering student from Nigeria in the MDevEng’s Healthcare Transformations track. In addition to her biomedical background, before coming to UC Berkeley Joshua spent four years involved in workforce development in Africa, where she helps women with digital skill training and job placement.
When looking at graduate programs, Joshua sought something that would allow her to combine three elements: social development, non-profit management, and inclusion. “I sought a curriculum that is immersive in managing and driving change from a global perspective and that looks at development from a social enterprise perspective,” she says. “And, because of my background in both healthcare and workforce development, I wanted a program that was interdisciplinary. When I found the MDevEng program, I was like ‘This is it!’”
Joshua began her workforce-development initiative after experiencing a trying period of her life. “I realized the African society I was in was not kind to helpless women and didn’t care about what you had been through,” she says. As a therapeutic activity, she would make animations for her son, using free, open-source apps. Not only did her son love them, but so did her followers on social media. Soon, businesses were asking her to do storytelling videos for their brands. “They were asking for my videos instead of my résumé,” she says. “Nobody was asking if I was male or female. Or if I was married or divorced. All they needed to see was my portfolio and that I did a great job and could deliver.”
After a few jobs, Joshua was able to purchase a laptop and establish a successful online brand. Then, in 2020, dozens of people asked her for help in moving their businesses online to keep afloat during the pandemic. That’s when she realized the need for digital skills, especially among women to bridge this gap
Currently, Joshua trains women in English-speaking African countries, though she plans to expand to Francophone ones soon. The training ranges from basic computer skills to advanced skills like UI/UX design to software development. “I realized the issue of high unemployment amongst women wasn’t a lack of jobs,” she says, “but more of underemployment and the lack of employable skills.”
Her first training was with 35 women. Within only a few years, she says, she has empowered over 8,000 African women from across 35 countries to earn their own money and become self-sustainable by leveraging digital skills.
“Students in GPP and DevEng are building their knowledge and skills about effective approaches to addressing poverty every day,” says Chetan Chowdhry, the Blum Center’s director of student programs. “They are thinking critically about how they can use their position as UC Berkeley students and soon-to-be alumni to support marginalized communities in ways that are respectful, ethical, and sustainable.”
Passion has led Praphanphoj to join the Master of Development Engineering program at UC Berkeley, where he focuses on sustainable design innovations. In his third and final semester now, he says he has enjoyed learning global development history and issues.
With his passion for design and cars, studying automotive engineering came naturally for Pun Praphanphoj when he started college. Originally from Thailand, Praphanphoj spent his college years at the HAN University of Applied Sciences in the Netherlands. There, he equipped himself with knowledge and skills in mechanical engineering and gained practical experience, from building a racing car for Formula Student Competition to interning in the fuel cell industry in Europe.
Praphanphoj was determined to work in the car industry when graduating from college. However, after returning to Thailand and working at Toyota on developing embedded systems and autonomous vehicles for almost two years, he reconsidered. “I wanted to have more impact and not be like a cog in a machine,” Praphanphoj says, recalling why he was motivated to leave the car industry for a while and try something new.
This led him to Energy Absolute PCL, a renewable energy service provider in Bangkok. Praphanphoj worked as a project manager designing greenhouses for farmers in the local area to grow organic vegetables, as well as designing battery-powered locomotives. The company had a dozen greenhouses where it partnered up with the farmers and sponsored them with equipment, seeds, and a market to sell these vegetables. For one particular project, Praphanphoj programmed a farming system that could control each crop’s condition individually and report plant conditions online, helping farmers better monitor and manage their crops. The experience taught him the importance of engaging with people and learning about their needs when designing projects. It also prompted him to pivot from an engineering role to pursuing a growing passion for bringing technological solutions to societal and environmental problems.
Praphanphoj (white shirt) working at a greenhouse in Bangkok with Energy Absolute PLC (courtesy photo)
“This experience also made me realize that engineering and tech alone will never solve any human complex issue without considering other aspects of the problem,” he says. “It converted me from truly believing in the power of tech alone to be more humble and holistic in my approach towards problem solving.”
This passion has led Praphanphoj to join the Master of Development Engineering program at UC Berkeley, where he focuses on sustainable design innovations. In his third and final semester now, he says he has enjoyed learning global development history and issues. Through taking classes including DevEng 202: Critical Systems of Development, he became more aware of the more nuanced aspects of global development — and the long-lasting impacts development engineering could have on people and their communities.
“They ground you in the knowledge that there are people not only working for monetary purposes, but for improving other people’s lives as well,” he says.
Whether it’s with professors who’ve been doing the work of development engineering for decades or with fellow students from different backgrounds and countries, Praphanphoj says he values having conversations about how things should be done to create impact and change the status quo. With the MDevEng’s wide range of elective classes, he also took courses in other departments, learning innovative finance for development and natural climate solutions and global change.
For a project-driven class, Praphanphoj took part in a project with Maia Africa, a Burkina Faso company specializing in producing mosquito-repellent products. Such products are particularly essential in regions of West Africa where the prevalence of malaria makes the local population vulnerable to mosquito-borne diseases.
The company had already introduced a mosquito-repellent ointment to the market. However, they sought a more innovative solution to disrupt the mosquito reproductive cycle directly. This is where Praphanphoj and his three teammates stepped in, devising a strategy to impede mosquito egg-laying, thereby curbing the growth of the mosquito population. They came up with a low-maintenance, low-cost, and water-based trap, which would lure female mosquitoes to come in and lay their eggs. While the product has not entered the production phase yet, Praphanphoj appreciated learning the process of designing this solution, along with the chance to present an economical and innovative technology to address a longstanding issue in the region.
Praphanphoj says growing up in Thailand and studying and working in Europe and the U.S. have shaped him into a flexible and open-minded person. “I think the ability to embrace and see things as they are and not imposing how things should be done is something that I’ve learned through traveling, studying and working in different places,” he says. “That’s a quality that I’m quite proud of.”
Such experiences enrich and shape Praphanphoj’s professional perspective as an engineer as well. He believes engineers should not only rely on their own past experiences and knowledge, but also listen to local people and learn from their experience about what the solution should be.
“You need to make sure that you’re not playing the savior role here and trying to push whatever you think is best for them, but rather be someone who’s there to listen and accommodate what they want and make sure whatever you offer fits within the context of how they live,” he says.
This summer, Praphanphoj was selected as an Engineering for Change fellow and currently works for Good Machine as a prototype engineer. He contributes to a project using observational balloons to track natural disasters in California. The team is now developing a system for balloon control at different altitudes while building additional testing capacity for system-level testing.
Praphanphoj with a prototype of a race-car frame (courtesy photo)
And for his MDevEng capstone project, Praphanphoj is working with Takataka Plastics, a start-up co-founded by a Berkeley mechanical engineering and DevEng alum providing waste management solutions. His specific project addresses recycling issues in Uganda by optimizing the placement and frequency of the pickup locations of plastic collection bins around the city of Gulu. By the end of the fall semester, Praphanphoj will present the company with a recommendation to improve the program’s logistics and engage more residents to participate.
Praphanphoj sees himself as a creator and designer who wants to use his skills to develop solutions or products that would be helpful to low-resource communities. After graduating in December, Praphanphoj says he’s interested in working in the renewable energy space, as well as in carbon capture and sequestration. Specifically, he wants to prototype and have fun in early-stage product development — something that hasn’t changed since his days building race cars.
Paige Balcom, the co-founder, co-CEO and CTO of Takataka Plastics, is changing Uganda — one plastic bottle at a time.
Paige Balcom, the co-founder, co-CEO and CTO of Takataka Plastics, is changing Uganda — one plastic bottle at a time.
In 2017, Balcom, who earned her Ph.D. in mechanical engineering at the University of California, Berkeley, was settling into campus life after spending a year in Uganda on a Fulbright research grant. Only a month into her first semester, Balcom heard about the Rudd Family Foundation Big Ideas Contest, which encourages and empowers students to solve social issues. She knew she wanted to get involved, but was initially stumped for a meaningful idea. While talking to her father about potential research topics, however, he reminded her about the pollution problems they had both witnessed in Gulu, Uganda. Plastic waste is a significant problem there, affecting the environment, people, and ecosystems, she says.
“The streets are full of trash — full of plastic waste — and a lot of it was burned too, creating soot and air pollution and toxic fumes. I wanted to make sure that Ugandans also thought it was a problem, so I started talking to some Ugandan friends. They agreed that plastic waste is a really big issue,” Balcom explains. Once she found the problem she wanted to solve, she formed a team with other students on campus. “We went to the library one Saturday morning less than a week before the Big Ideas proposal was due, and just sat there for hours doing a brainstorming session,” she adds.
The beginnings of Takataka Plastics came together during that long Saturday among the stacks. The team came up with a company name, Trash to Tiles, and envisioned a process where polyethylene terephthalate (PET) plastic bottles — the kind used for bottling water and soda — would be transformed into usable products such as building tiles and furniture. The process would also aid people in the community by creating jobs and income.
Balcom’s experience is a textbook example of the social innovation that the Big Ideas ecosystem catalyzes. Click here to read more about how the program has supported over 9,000 students, through the stories of Paige and two other social innovators who have transformed their Big Ideas into real-world impact.
On Aug. 22, the third cohort of the Master of Development Engineering program convened at Blum Hall for their orientation and the start of the first of three semesters of an interdisciplinary curriculum that revolves around developing technology interventions in accordance with and for individuals living in low-resource settings. The Class of 2024 — 34 students in total — hails from 12 countries across four continents, but many arrived last week for breakfast and headshots already on friendly terms.
Every August marks the arrival of fresh faces at UC Berkeley, and for the third year running, some of those new students will be earning the country’s — if not the world’s — first graduate degree in Development Engineering.
On Aug. 22, the third cohort of the Master of Development Engineering program convened at Blum Hall for their orientation and the start of the first of three semesters of an interdisciplinary curriculum that revolves around developing technology interventions in accordance with and for individuals living in low-resource settings. The Class of 2024 — 34 students in total — hails from 12 countries across four continents, but many arrived last week for breakfast and headshots already on friendly terms.
In addition to being students in the burgeoning field that first coalesced at Berkeley, the cohort will also be active practitioners and shapers of it. When digitally polled about what they thought “Development Engineering” means, “dignity” was the first reply to hit the giant screen of Blum Hall B100. “Flourishing” and “communities” were early leaders in the live word cloud, but “innovation,” “technology,” and “sustainable” became three of the class’ most dominant perspectives on their new area of study and practice.
The appearance of “diversity” prompted a discussion that got at the heart of DevEng. Hussein Orekoya, a civil engineer from Nigeria, elaborated: Diversity in innovation, he said, meant recognizing that “a solution that might work here in California might not work in Africa.”
In addition to working in civil engineering in Lagos, Orekoya is the founder and executive director of My Environment is Mine Initiative, a youth-led organization promoting sustainable development across the continent and guided by the UN’s Sustainable Development Goals. His classmates arrived in Berkeley having done everything from petroleum chemistry to AI and robotics in government.
The MDevEng Orientation scavenger hunt took new master’s students all over campus, including Doe Library. (Hussein Orekoya photo)
Following a round of icebreaker bingo — filling in squares by finding new classmates who fit criteria like owning a pet or starting their own social venture — the cohort broke off into groups for a campus-wide scavenger hunt, a particularly important geographical orientation considering their elective classes this fall span 10 departments.
That interdisciplinary breadth — and DevEng’s focus on the big-picture context of complex problems — make the MDevEng “the program I wish I could have taken when I was a student,” Prof. Kara Nelson, chair of the Graduate Group in Development Engineering, told the new cohort, which started classes the following day.
But students, she said, will have to pair tenacity with working in interdisciplinary teams and digging deeply to understand the local contexts of the problems they’re solving for. It’s not easy work, she warned. “You have to be fearless and never give up.”
“It’s so daunting,” Nelson said, “but it’s so fun.”
Yet even before AI took center stage this past year, students and alumni of the Blum Center for Developing Economies were embracing the emerging technologies’ potential, specifically for social good. From detecting “deepfake” videos to analyzing agriculture changes and building understanding across communities, Blum Center folks share their experiences, inspirations, and the impact of their AI-driven projects and ventures.
Only about a year has passed since DALL-E, the AI text-to-image model, and ChatGPT, the large language model–using chatbot, ushered in what feels like the age of AI: months of wall-to-wall news coverage of and personal experimentation with the most powerful publicly available artificial intelligence programs. But what started off as images of Darth Vader playing in the NBA and the near-instant generation of new bedtime stories have given way to concerns about how AI can contribute to disinformation campaigns, academic dishonesty, and even an end to whole classes of workers whose jobs can, theoretically, be done by machines.
Yet even before AI took center stage this past year, students and alumni of the Blum Center for Developing Economies were embracing the emerging technologies’ potential, specifically for social good. From detecting “deepfake” videos to analyzing agriculture changes and building understanding across communities, Blum Center folks share their experiences, inspirations, and the impact of their AI-driven projects and ventures.
Shaping the battle against deepfakes
Raymond Lee (courtesy photo)
Back in 2019, Raymond Lee, a former Big Ideas Contest winner and a UC Berkeley alum, spotted the growing threat caused by deepfakes — media created using learning techniques that can swap faces, voices, and even entire bodies, making it appear as if someone is saying or doing something they never actually did.
While deepfakes became viral and raised public concerns, no technical solutions stood out then. Lee decided to initiate FakeNetAI, a deepfake detection SaaS (Software as a Service) that aimed to “protect against economic, societal, and political threats.”
FakeNetAI began as Lee’s capstone project during his master’s program in data science, and it quickly evolved into a startup with the support of his teammates from data science, electrical engineering and computer science, and Haas MBA students. And through participating in the Big Ideas Contest, Lee connected with mentors, conducted market analysis, and developed a mature business plan.
To train their machine learning model, Lee and his teammates curated a diverse dataset by employing open-source data sets, scraping raw data from YouTube, and collecting deepfake videos created using various methods. The team’s approach and the customized machine-learning architecture resulted in a detection accuracy of over 90 percent.
Since its victory in the Big Ideas Contest in 2019, the startup has successfully attracted media outlets, banks, and social media firms as customers. For NewsMobile, an Indian fact-checking site, FakeNetAI helped identify viral deepfake videos featuring prominent figures like Tom Cruise and Donald Trump. Moreover, it aided in verifying livestreaming videos during a critical moment of the Myanmar coup for another third-party fact-checker.
However, Lee acknowledges that the fight against deepfakes is far from over. The rapid proliferation of deepfake generation has still outpaced the development of detection expertise. Citing the research of Prof. Hany Farid from Berkeley’s School of Information, Lee emphasizes the urgent need for continued research in detecting these highly realistic manipulated videos.
“It’s like a cat and mouse game where you constantly have to outsmart the generation models with your detection model,” he says.
The other challenge is, because media comes in a wide range of formats, it takes a lot of work to train a machine-learning model that can perform well on all different formats. So the more generalized a machine-learning model is made to be, the less accurate it becomes.
FakeNetAI is still growing, and Lee is determined to stay at the forefront of innovation. He has also pivoted his career to do more general AI and data science consulting. “The image generation field has advanced at a rapid rate,” he says, “and there’s always a lot of interesting stuff going on in the video, image and text generation space.”
Understanding abandonment in Ukrainian agriculture amidst war
Sarah Hartman, a PhD student within Environmental Science, Policy, and Management, has been involved in the Digital Transformation of Development traineeship since last year, and will continue as a funded fellow for this upcoming year.
Before joining DToD, Hartman’s research interests in food and water led her to participate in the InFEWS program. What she enjoys the most about these programs is the opportunity to interact with individuals from diverse backgrounds and disciplines.
“I’ve gained a lot intellectually by chatting with people,” Hartman says. “There were things that I learned from the other fellows that have helped reframe how I think about my research or have made me think about potential tools and methods that I hadn’t otherwise stumbled upon.”
In her research on water and agriculture, Hartman utilizes machine learning and AI to map changes and quantify the extent of agricultural activities. Her recent work involves training machine-learning models to analyze satellite images of Ukrainian agriculture during its war with Russia, with a specific focus on abandonment and its underlying drivers.
The idea stemmed from a teaching experience when Hartman was a graduate student instructor for a Principles of Natural Resource Management class. As the war in Ukraine began during the semester, she noticed the students’ desire to understand the global impact of such events on natural resources and supply chains. She then decided to deliver materials around globalization with a specific angle of Ukraine. For instance, the country is one of the world’s breadbaskets, where fields of sunflowers, wheat, and corn provide food for some of the world’s most water-stressed and vulnerable countries, particularly many in North Africa. The abandonment of Ukrainian fields could cause serious food instability for its importing countries.
Inspired by the dynamic conversations in class, Hartman wanted to pursue a research project on the issue. “I took it personally,” Hartman says. “I’ve been learning how to use satellite images and machine learning to look at agriculture; what better place to do it than to help inform what’s happening in Ukraine in near real-time?”
Are fields abandoned because of a physical tank or destruction? Or because of supply chain issues such as farmers unable to get sufficient fertilizer or no longer able to sell their crop? Hartman’s research looks into these issues by analyzing satellite images and hopes to reveal what affects the overall resilience of Ukrainian agriculture. Specifically, she analyzes historical and near-real-time satellite imagery in Google Earth Engine to map and categorize fields and landscapes to compare changes over time. She then relates these changes to other timestamped activities such as damage to transportation routes or local military activity.
Besides technical analysis, Hartman hopes she could do more outreach and engagement with local communities in Ukraine that are directly affected, which has been challenging given the ongoing war condition. She says she would love to work with organizations with access to the groups.
Hartman is captivated by the power of analyzing publicly available satellite images. She explains that researchers can access these images and gain insights into any part of the world, dating back to the 1980s or earlier. This accessibility proves particularly invaluable when collecting information on remote and resource-limited regions where data has historically been uncollected or lost.
“What an incredible opportunity to pair images that have been collected for tens and tens of years and use that to analyze things in a way that provides data that may not necessarily be possible otherwise,” Hartman says. “That’s what I see as the potential.”
Paving the way for empathy in the digital age
Kenan Carames, a current Master of Development Engineering student in the AI & Data Analytics for Social Impact concentration, is developing platforms that help people in different communities grow closer together in an online space. Already having a background in data analysis, he joined the program to pursue his interest in social issues and international development.
Kenan Carames (courtesy photo)
“There’s so much exciting stuff happening in AI both from a technical and social point of view,” he says. “And coming from an engineering background, I do have the opportunity to provide a more technical perspective in the social conversations.”
Over his two and counting semesters, Carames took classes on development issues and intense technical skills such as applied machine learning. A course called Politics of Information taught by Prof. AnnaLee Saxenian, also Carames’ mentor, sparked his interest in political issues around data and the social media space. His passion found a nurturing ground during his ongoing internship with Search for Common Ground Peace, a peacebuilding organization that aims to mediate conflicts and violent areas across the world.
Carames recently worked on developing a chatbot for the organization to guide individuals in countries including Sri Lanka, Nigeria, Kenya, Jordan, and Lebanon towards resources that promote empathy and mutual understanding. He primarily helped advance the user experience of the chatbot, which requires a lot of data analysis and visualization of how users interact with the product and which materials get the most engagement. The current structure of the chatbot is more like a decision tree or choose-your-own-adventure, Carames explains, but his team plans to use more natural language processing (NLP) to make it more dynamic and engaging in the future.
“It’s definitely different work than I’ve done previously. And it’s kind of cool to have these social goals that you’re working towards,” he says. “That feels very impactful.”
While Carames is still developing his MDevEng capstone project idea, he is determined to keep exploring efforts to build empathy in digital spaces. The concept of the project will be based on contact theory, he says. The theory holds that contact between two groups can promote tolerance and acceptance under appropriate conditions, and he wants to experiment with it in an online space.
From an engineering perspective, Carames will explore the system design and algorithm decisions he could make to ensure that when people from different groups come in contact with each other, they’re fostering understanding of each other rather than developing prejudice and hate. He has been learning from a project where researchers use question-and-answer website Quora to facilitate conversations about Israel and Palestine for people living in and outside these areas.
“It’s a very heated topic, and how do you set up those spaces and design conversations to get people to engage each other in a helpful way?” he asked. “It’s very difficult and messy, but I think that’s why it’s interesting.”
Xhafa has worked in the development sector for a decade and graduated from the Master of Development Engineering program last December with a focus on energy and environment. The intersection of healthcare and energy was also the focus of another recent MDevEng graduate, Greg Berger. Together, Berger and Xhafa, both in the program’s Energy, Water, and the Environment track, examined the energy needs of healthcare clinics in one sub-Saharan country, Rwanda, as their MDevEng capstone project.
Health care is a basic human right and a core resource for achieving the UN-adopted Sustainable Development Goals. But fully sixty percent, or roughly 100,000, healthcare facilities across sub-Saharan Africa do not have access to reliable electricity, or to electricity at all.
There is a well-documented correlation between energy access and positive health outcomes, a key reason why governments and development practitioners have committed to achieving universal electrification of health facilities by 2030.
This problem is right up Ingrid Xhafa’s alley. Xhafa has worked in the development sector for a decade and graduated from the Master of Development Engineering program last December with a focus on energy and environment. The intersection of healthcare and energy was also the focus of another recent MDevEng graduate, Greg Berger. Together, Berger and Xhafa, both in the program’s Energy, Water, and the Environment track, examined the energy needs of healthcare clinics in one sub-Saharan country, Rwanda, as their MDevEng capstone project.
Berger has always had a profound interest in energy. With a background in mechanical engineering, he plans to use his education to implement sustainable energy technologies in an equitable way. “Energy is pivotal to the foundation of modern human activities,” he says. “And it’s important to implement sustainable solutions by working with communities that did the least to contribute to the climate crisis but are hit the worst.” Xhafa, on the other hand, came in with a master’s in public policy and knows the impact policy has on resource allocation in energy and elsewhere.
An off-grid solar-power system
In Rwanda, Berger and Xhafa worked with Daniel Kammen, Professor of Energy and head of Berkeley’s Renewable and Appropriate Energy Laboratory (RAEL), who has long worked on evaluating the potential for off-grid power in the country and other nations in sub-Saharan Africa. Kammen became their MDevEng capstone advisor and helped kickstart the project by guiding research and remote work.
During the spring of 2022, Berger and Xhafa examined how Rwanda’s challenges with access to energy in remote areas have led to the implementation of new infrastructure such as off-the-grid systems that rely on solar panels to power small and medium-sized needs. Standalone off-grid solar has the potential to improve health services in remote villages with insufficient grid infrastructure. However, historically, most of these interventions have happened as ad-hoc initiatives from outside development practitioners, and the infrastructure’s maturity and sustainability has to be vetted.
Trained as engineers, but now with training in low-resource settings, both Xhafa and Berger knew these solutions needed to be assessed from multiple perspectives: technical robustness and feasibility, business model sustainability, and socio-cultural impacts. “The MDevEng program played a huge role in how I look at development interventions, as well as challenges to look out for in implementation,” says Berger.
Throughout their program, Berger and Xhafa worked with RAEL to analyze data from remote monitors placed in six Rwandan healthcare facilities to assess power quality and reliability generated by standalone solar boxes. PhD student Samuel Miles from RAEL had added remote sensors to them over a year ago to collect data on how well the stand-alone systems were operating in the country, without the need for someone to be constantly on-site to check. From there, Berger and Xhafa conducted in-depth analyses, asking questions like, “Does the existing energy system fulfill the needs of the clinic?” and “Are there more opportunities or challenges for more electricity?” and “Are there power disruptions throughout the day that are detrimental to the clinic?”
Inside a healthcare clinic
But this technical analysis alone doesn’t paint the full picture of what leads to the success or failure of an intervention. Berger and Xhafa needed to have on-the-ground discussions with clinic staff and community members to gather insights about the impact of this technology in the day-to-day. Last summer, the researchers spent a month in Rwanda examining eight health clinics, six of which had off-grid solar boxes installed with USAID support that provide solar power and clean drinking water to their facilities. The other two clinics were connected to the traditional power grid — a comparison point for understanding how the solar boxes’ electricity systems performed.
The duo recalls their journey in the country filled with surprises, from four car breakdowns to the incredible hospitality of the Rwandan people and extremely easy collaboration with the local staff. On a day-to-day basis, Berger and Xhafa coordinated with locals to visit those eight healthcare facilities, and with the help of a local translator, they spoke with the head of each one, as well as their nurses and doctors, to grasp the specialized needs and testimonies of each clinic. They toured the clinics to conduct inventory, perform basic energy audits and analysis, and provided clinic staff with a survey to obtain measurable data.
Xhafa and Berger meet with a clinic staffer
They found that most of these standalone systems provided quality power when operable, however differing clinic needs led to different levels of power consumption and down time. On top of that, the clinics were largely unable to fulfill their other objectives of providing electricity and water services to the community in a financially feasible way for the system operations.
The RAEL team concluded that the intervention had poor site selection from the beginning; areas were not densely populated enough to earn revenue from the productive use of electricity. On top of that, these standalone solar solutions did not consider the arrival of government-provided grid infrastructure which would negate the need for standalone systems. Plus, Xhafa says, “one solution fits all” may not be the best approach for all energy projects in Africa.
They also found the system sizing to be generic and that seasonal factors made a big difference in power adequacy. Involving the communities in the design and implementation processes could have avoided some of these problems. “We noted a lack of adequate training on system operation and uncertainty of how these systems will be sustainable once the equipment starts aging or when technical issues arise,” Berger says.
By the end, Berger and Xhafa, in conjunction with RAEL, quantitatively showed the challenges of a one-size-fits-all power system, and they hope these insights can provide some crucial information for similar initiatives. Standalone energy systems can be vital in remote areas with no grid reach, they say, but alternative financial models have to be explored and the economics behind the productive use of electricity understood.
Being trained with this mindset through the MDevEng program, the pair put a greater emphasis on the clinics’ communities, considering them as the customer of the solution and treating their testimonials as valuable insights alongside the hard data. Both Xhafa and Berger highlighted how valuable it was to have the community at the center of their research.
“They are hardworking and ingenious people who can solve their own problems,” Xhafa says. “The solutions suggested by the locals have the highest opportunity to be successful.”
The past year also witnessed momentous firsts in our Development Engineering community and some impressive triumphs by students well on their ways to making tangible impacts on real-world problems.
This past academic year has, dare we say it, felt more or less normal. We were, in a most literal sense, finally and consistently together again.
After what felt like ages in a pandemic bubble of Zoom classes, working from home, and frightful news headlines, the Blum Center and Berkeley campus have returned to a state of relative and in-person normalcy: classrooms returning to capacity, events at Blum Hall multiplying, rediscovering the delight of cake and coffee at a staff meeting. While we remain vigilant in our health precautions, May 2023, the final month of the academic year, saw the end of COVID-19 as a WHO global health emergency — a hopeful coda to 2022–23.
The past year also witnessed momentous firsts in our Development Engineering community and some impressive triumphs by students well on their ways to making tangible impacts on real-world problems. Below are some highlights.
In August, the second-ever cohort of our Master of Development Engineering program arrived at Blum Hall to begin their three semesters of study. Hailing from 10 different countries, the class came in with experience in everything from designing shelters for victims of gender-based violence in remote villages in Indonesia, to prototyping and testing affordable greenhouses for hundreds of smallholder farmers in India, to developing solar power projects in Peru and Tanzania.
The three dozen new grad students all seemed to agree on one thing at their Aug. 23 orientation, however: “The food in Berkeley is so good!”
In September, economics professor and our chief economist Brad DeLong published Slouching Towards Utopia, an expansive account of the economic history and technological changes from 1870 to 2010, surveying “the monumental transformations — and failed promises — brought about by an extraordinary rise in prosperity.”
“While the past 150 years have solved the problem of baking a large enough economic pie for everyone to potentially have enough,” DeLong said, “the problems of properly slicing and then enjoying that potentially ample economic pie have flummoxed us as a species.”
The Financial Times and The Economist named Slouching Towards Utopia one of their best books of 2022.
Speaking of books, a mere three days after DeLong’s book debuted, the first-ever textbook dedicated to Development Engineering hit publisher Springer’s website.
The book features 19 case-study projects, from fintech for rural markets in sub-Saharan Africa to stopping arsenic poisoning in India to protecting electoral integrity in emerging democracies, along with four framework chapters on the field’s history, ethical challenges, and philosophical roots.
In December, the inaugural MDevEng cohort received the U.S.’s (if not the world’s) first master’s degrees in Development Engineering. In designing and implementing interventions in accordance with and for people in low-resource settings, the 44 students’ capstone projects included a business for seamstresses in rural Ghana to sell their high-quality wares, advancing an initiative to bring arsenic-safe drinking water to rural cities in California, and a blockchain-certified recruiting platform enabling Nigerian students to close the gap between job seekers and employers.
“You have become the precedent for what this program can and will become: a program marked by educating and equipping changemakers to develop innovative global solutions,” said commencement speaker Prof. Maya Carrasquillo. “What a powerful vision, and each of you embodies that so much.”
Kara Nelson named head of the Graduate Group in Development Engineering
Prof. Nelson took over from retiring mechanical engineering Prof. Alice Agogino, a key force behind the creation of our DevEng programs who also served, among many other positions and distinctions, as the Blum Center’s education director and leader of the MDevEng’s Sustainable Design Innovations track.
…High Tide, a Berkeley student duo replacing plastic coatings with bio-based coatings for single-use products that allow them to be composted and recycled. Of the 23 finalists at May 3’s Big Ideas Grand Prize Pitch Day at Blum Hall, judges awarded Ivan Jayapurna and Kira Erickson the $10,000 grand prize.
“The concept behind High Tide was born out of a realization that the majority of our paper products are destined for landfill, despite paper being a compostable and recyclable material,” Erickson said. “It’s an extremely pervasive yet less widely known issue. The potential for systemic impact is massive if addressed properly.”
2ndWind, which assists small- and medium-sized businesses once their owners retire, earned the Lab for Inclusive FinTech (LIFT) “FinTech for Social Good” Initiative award.
Sixty more students — all of whom had to adapt their studies and practice experiences to pandemic-caused restrictions — joined the GPP minor’s 1,000-plus–member alumni community on May 15 in a commencement ceremony infused with gratitude and optimism.
“There is so much power in recognizing the process of working for change as its own reward: All one has to do is stay the course, regardless of where the path leads,” said one student speaker, Samyukta Shrivatsa.
“GPP has been a process of tearing down everything we thought we knew about the world and rewriting the stories we tell about it,” she told her peers. And the story that GPP tells?
“One of audacious hope in the world and each other.”
Thank you to our students!
We’ve had the honor of directly serving more than 1,000 undergraduate and graduate students this year — practitioners of poverty alleviation, health-technology innovators, development engineers, social entrepreneurs, and more. And we look forward to serving many more in 2023–24! Please let us know how we can help.
Hebee is one of two Berkeley student teams that developed their innovations over the past year through the Health Tech CoLab, an ecosystem to support students developing medical devices, diagnostic tools, and digital health tools that increase access to healthcare. The CoLab’s Health Access Cohort also included Diaita, which offers personalized diet and exercise plans as well as cognitive behavior therapy to ward off Type 2 diabetes and its associated illnesses.
Berkeley students Paige Lyles, Megan Chan, and Ariana Satari know what it’s like to start their periods unprepared: “the feelings of panic and stress that flood your chest as you have to drop what you’re doing and rush to find a solution,” says Lyles.
But despite periods being a natural bodily function, the lack of access to period products in public places (not to mention the lack of education around menstruation) leaves many people in this very position — even while toilet paper and tissues are provided in public restrooms without a second thought. “Period poverty” affects everyone, Lyles, Chan, and Satari point out: from unhoused people to “working students and parents who have to choose between buying food and buying increasingly expensive period products.”
That’s why Lyles, who studies civil and environmental engineering, and Chan and Satari, mechanical engineering, founded Hebee, a smart period-products dispenser and mobile app for school campuses where both menstruators and facilities staff can see on the app where dispensers are located and exactly how many pads and tampons are stocked in each. One of its unique innovations is a universal wall that can expand or contract to fit products of varying size.
Hebee is one of two Berkeley student teams that developed their innovations over the past year through the Health Tech CoLab, an ecosystem to support students developing medical devices, diagnostic tools, and digital health tools that increase access to healthcare. The CoLab’s Health Access Cohort also included Diaita, which offers personalized diet and exercise plans as well as cognitive behavior therapy to ward off Type 2 diabetes and its associated illnesses.
“These teams are not only examples of clever product innovation, but they epitomize what it means to be social innovators,” says CoLab manager Karenna Rehorn. “They’re motivated and guided first and foremost by wanting to improve people’s health and lives and to address glaring social and health disparities.”
Being a part of the Health Access Cohort, says Diaita cofounder Ariel Ho, a registered dietician from Taiwan and Biomedical Visiting Scholar at Berkeley, “has given the team the chance to participate in various workshops on customer discovery, prototyping, user testing, and pitch development.” The CoLab, she adds, “has provided Diaita with opportunities to connect with academic and industry experts to gain insights into how to build a product that better fits user needs and furthers healthcare access.”
Ariel Ho (Diaita photo)
Ho founded Diaita a year ago. Like the Hebee team, they noticed a glaring gap in a field of healthcare and access: the “need for a digital health intervention that provided prediabetic individuals with personalized, flexible, culturally responsive diet and activity suggestions with an emphasis on long-term, sustainable behavior change.”
As CoLab residents, Ho and collaborators Midori Pierce, a Master of Information Management Systems student, and Meng-Chia Chiang, in the Haas Global Diploma Program in Entrepreneurship and Innovation, conducted more than 100 interviews to understand potential users’ needs in order to determine product-market fit, performed in-depth testing of their user interface and user experience designs, and prototyped their app. True to the CoLab’s mission of using collaboration and networking as engines of health-tech innovation, they linked up with medical professionals, insurance industry experts, investors, and researchers.
During their CoLab tenure, the Diaita team learned that they need not have a perfect “minimum viable product” from the get-go, but rather a solid one that can be refined over time. Originally, they had wanted to incorporate machine learning and a wearable device, but reconsidered those ideas as long-term goals. They also learned, as Ho said, to “communicate effectively through differences and use their diverse skill sets and perspectives” to work through clashing opinions on product design — something that naturally arises out of a team with such diverse professional backgrounds.
The Diaita team recalled “deeply personal and heartfelt” stories from their customer-discovery interviews about their experiences with diabetes-related problems — and interviewees’ enthusiasm for Diaita’s innovation.
“Hearing these stories has kept the team motivated week after week and month after month to continue on with this very important work, knowing that there are so many individuals who can benefit from Diaita’s health-tech solution,” Ho said.
Diaita plans to soon release an initial version of its product through Apple’s App Store and the Google Play Store, while continuing to interview stakeholders, iterate their product, and network, with the hopes of raising capital, growing their customer base across new countries, “pursuing clinical validation through research,” and reviving that original concept of integrating a wearable device.
Hebee, founded in 2021, also used its CoLab membership to develop multiple iterations of its dispenser, including with help from the Jacobs Hall Makerspace and its 3-D printers, laser cutters, and other tools they could access at no extra cost. The team also gained valuable insight from the CoLab’s diversity, equity, and inclusion activities, going on to partner with community and student organizations in the Bay Area to obtain and give out period products to those in need.
“We as a team have benefited from DEI workshops to ensure that our brand continues to uphold these values through the way we iterate our product and how our presence is cultivated within the community,” Lyles said.
Earlier in their residency, with help from Rehorn and their mentor Cathy Farmer, they figured out an effective user-testing plan, despite not yet having a fully functional prototype to try out on campus. Now, Lyles, Chan, and Satari are preparing to launch both their user-testing and their dispenser and app prototypes across the Cal campus — with app-development help from two “brilliant” interns, Andres Lam and Yugam Surana.
“The energy in the CoLab space is positive, and makes working enjoyable for us,” Lyles says. And that even includes a small kitchen where they can keep and prepare food on their longest working days. “It makes the student-founder balance a lot more manageable. Having a supportive community is especially important when you are in the early stages of development.”
In the fall of 2021, Master of Development Engineering students Victor Okoro, Daniel Huang, and Joshua Iokua Albano, interested in education and helping Nigerians find jobs post-graduation, teamed up to found Madojo, a platform that connects Nigerian university graduates with employers in the technology space while helping the graduates gain sought-after skills through skills development, portfolio design, networking, and mentorship.
Nigeria is home to by far the highest number of startups in Africa, and over the past few years, these startups have received a large amount of venture funding — over $1 billion in 2022 by one estimate. These startups are looking to hire a local workforce, but a stark difference exists between the skills employers look for and the skills Nigerian applicants have when they graduate from universities.
In the fall of 2021, Master of Development Engineering students Victor Okoro, Daniel Huang, and Joshua Iokua Albano, interested in education and helping Nigerians find jobs post-graduation, teamed up to found Madojo, a platform that connects Nigerian university graduates with employers in the technology space while helping the graduates gain sought-after skills through skills development, portfolio design, networking, and mentorship.
The team came to the MDevEng program from different career fields. Okoro, a native of Nigeria, worked in software engineering, and most recently as a technology architect. Huang’s background is in entrepreneurship, product development, and security consultancy. Albano has worked in machine learning and data engineering.
The three channel all this experience into Madojo. Okoro, the team’s executive officer, was born and raised in Nigeria, has a personal understanding of the job market and economy of the country, and serves as the point of contact for Nigerian employers and students. Huang, Madojo’s technology lead, uses his product-development experience to design their curriculum. And coming from an engineering and design background, Albano has taken responsibility for the presentations and reports that Madojo puts out.
Madojo is a “hybrid learning community that connects employers with university students in Nigeria,” Huang says. “The goal is to be able to close the experience gap that students have before starting their first job.” In Nigeria, students have access to experiential learning opportunities such as internships and undergraduate research positions, “but the overall economic structure is not robust enough to support them extensively, ” Okoro says. There is a need to democratize skills such as coding and writing computer programs because only a small percentage of university students follow through and learn these skills before entering the workforce.
At the end of 2021, the Madojo team decided to apply to the Big Ideas Contest to move their idea forward. The competition provided critical structure, accountability, mentorship, and feedback. Albano found the process of pitching their project to be most beneficial because it taught the team how to “convince others that do not have the context or background [the team has] that this problem needs to be solved.”
They were able to do just that. In the spring of 2022, judges awarded Madojo the first-ever Binance Charity–LIFT Initiative Award. The LIFT FinTech for Social Good Initiative, a parallel contest to Big Ideas’ flagship competition, seeks to support students working on financial technology ideas to advance social change by unlocking the potential of these digital technologies to benefit underserved populations around the world—the very goal of Berkeley’s Lab for Inclusive FinTech (LIFT), which focuses on research, experiential learning, and community building. “What better way to do this than by organizing a contest in which we focus specifically on financial technologies or blockchain solutions that are able to make an impact on people’s lives,” says Laura Chioda, the director of research at LIFT and the Institute for Business and Social Impact at the Haas School of Business. The FinTech for Social Good Initiative is made possible by the generosity of Binance Charity and Ripple Impact.
Madojo “provides students professional experiences in a setting that allows them to get feedback in terms of the professional skills, technical skills, collaboration skills,” Huang says. “This format will also serve as a recruiting platform for employers.” To this end, Madojo’s curriculum has two main topics of emphasis: technical skills and professional development. Students learn technical skills through case challenges based on local Nigerian problems that teach students how to utilize data to solve those problems. These case challenges help students develop “microcredentials,” which allow them to show an in-depth understanding of a particular topic or skill that is relevant to future employment opportunities. In this way, the platform streamlines the recruiting process for employers, who can see these skills, while giving applicants real-world experience. Students also focus on developing professional skills such as how to give elevator pitches, how to write resumes and cover letters, and how to find and apply for jobs. “At the core of what we’re doing is walking the students through how to problem solve,” Okoro says, because this is a large focus of employers in Nigeria.
Although the Madojo team does not yet have a platform available, they are connecting with students all over the country through Google Forms and email. At the end of last year, Madojo ran a pilot program with 15 Nigerian students, who were enrolled in a 10-week, microcredentialing course that the team designed to gauge their interest in the program and see if the program benefits them. The team sees Madojo as a community and hopes members will utilize its curriculum to become career self-starters. “We’re only successful if [students] are able to take away all the skills, networks, and connections” that they are offered, Huang says.
In the future, the team hopes to digitize the program, drawing inspiration from Nigerian career portal Jobberman and Kaggle, an online community of data scientists. They want to create a platform “where students can upskill, verify the skills they have, and upload those skills to their portfolio,” Albano says. This would allow students to have one webpage where they can display their resumes, portfolios, and other products or code they have written.
The name “Madojo” comes from combining the word for “community” in the three main Nigerian languages, Hausa, Yoruba, and Igbo. To the team, which graduated from the MDevEng program in December, “the most important thing is building a community of learning and a community of opportunities,” Okoro says. As with many promising technologies, Madojo’s users will also put it to use for a more diverse array of purposes than the founders imagined, from addressing climate change to working with youth to even owning a dance company to put on performances for the community.
“They are really community focused,” Okoro says. “They are looking to give back to their communities with the opportunities and resources to do so.”
As a senior program manager at Institute for the Future, a non-profit encouraging individuals and organizations to plan for the long-term, Lipsett looks at the world-to-come through a collaborative lens. But her dedication to innovative futures transcends her office. As a judge and mentor of the Big Ideas Contest, housed at the Blum Center for Developing Economies, Lipsett has become a key piece of the program and an exemplar for students who too hope to redesign how we approach forthcoming generations.
When we think about our socio-economic future, endless possibilities come to mind. You may be concerned about the changing climate or advancements in technology or how various social groups interact with each other. Or maybe you’re thinking on a smaller scale, interested in how your community will be affected. Ilana Lipsett explores all of these facets. As a senior program manager at Institute for the Future, a non-profit encouraging individuals and organizations to plan for the long-term, Lipsett looks at the world-to-come through a collaborative lens. But her dedication to innovative futures transcends her office. As a judge and mentor of the Big Ideas Contest, housed at the Blum Center for Developing Economies, Lipsett has become a key piece of the program and an exemplar for students who too hope to redesign how we approach forthcoming generations.
Lipsett is a Bay Area native, born and raised in the East Bay, and frequented UC Berkeley for summer school growing up. She attended college across the state at UC San Diego, studying History, French Literature, and Music. Her unique educational focuses led her down a long and windy road of various disciplines: She started off in Washington, D.C. at the intersection of labor and politics, working on everything from political campaigns to advocacy work for displaced workers. Ten years later, she returned to the Bay Area to get her M.B.A. in Sustainable Management at Presidio Graduate School. During and after grad school, Lipsett worked for the City of San Francisco at the Mayor’s Office of Economic and Workforce Development. This kickstarted her work in urban development with an emphasis in community engagement; her advocacy for creating accessible and inclusive public spaces and public-facing activities translated across different domains: from the City of San Francisco, to a private real estate developer, to her own business, and even at an international scale, supporting community spaces in refugee camps.
Now, Lipsett advances her brand of public engagement and participatory design at the Institute for the Future (IFTF). Her work has a civic-futures focus, entwining sustainable community solutions into everything from political systems to real estate. One of her many ongoing projects works to expand a predominantly POC housing co-op in San Francisco by creating an accessible STEM center and Performing Arts Center in unoccupied buildings. But Lipsett also values impact through education. At IFTF, Lipsett teaches public classes to an international audience on design futures and foresight essentials. “I really want to give people the tools to think about how the future can be different,” she says. “Then encourage them to get creative and make the changes so they can move towards their preferred future.” Lipsett certainly practices what she preaches: As a singer and songwriter for “The Seastars,” a girl band that uses music to advocate for a climate sustainable future, Lipsett taps into her creative side to encourage others to change their behavior in favor of our environment.
When she is not busy changing the future and using music to empower the world, Lipsett carries teams to victory in the annual Big Ideas competition. Lipsett first heard about Big Ideas in 2018 through her friend, Dani Bicknell, a program manager for Big Ideas at the time. Bicknell told her about the competition and asked if she wanted to be a part of it. “I always love to be involved in the local community, but Big Ideas especially felt like a great fit with the skills I have to offer and how I want to be connecting with others,” Lipsett says. So, on whim, she said yes, but just as a one-time commitment. But that one time, where she served as both a judge and a mentor to a team, was such an incredible experience that she immediately knew that it wouldn’t be her last. “It was such an amazing opportunity to see students see potential in something new,” she says.
As a judge, Lipsett reads and judges student entrants’ social innovations’ pre-proposals based on a specific scorecard, deciding whether it should move on to the final round. There are four factors on which pre-proposals are measured: viability, originality, team, and quality. “Saying no is probably the hardest part,” she admits. “Every proposal is so interesting and creative.” After the finalists have been determined, Lipsett is matched with a team of students to act as their mentor. Lipsett highlights how perfectly aligned she was with teams she was matched with. For example, one project she mentored, Doin’ Good, aimed to provide vocational education to Syrian refugees in Lebanon by creating mobile maker spaces and education centers out of a van. Conveniently, Lipsett had just come back from Bangladesh, creating maker spaces at refugee camps there. And Lipsett’s expertise certainly paid off — Doin’ Good won first in the Workforce Development track in 2019 and was a Grand Prize finalist!
As a mentor, Lipsett meets with her mentees every week, setting a timeline of work to be done and anticipating and preemptively addressing potential challenges or gaps. From providing connections to people working in the field to helping with the budget, Lipsett was the go-to person whenever her team was stuck. But Lipsett believes it’s the students’ drive that allows the project to flourish. One team Lipsett mentored, Send Help, proposed an AI chatbot that connects citizens with police alternatives during non-emergencies. Essentially, they wanted to make calling non-police first responders as easy as calling 911. Lipsett suggested to the team that the proposal needed an endorsement from public officials, and the next thing she knew, the team had met with the Berkeley City Council and got letters of approval from policymakers.
Lipsett is certainly not short of accolades in her own endeavors for innovative change. In 2013, the White House awarded the Champion of Change Award to her and her team for creating [freespace], a movement dedicated to activating vacant spaces as temporary community, cultural, and art hubs. [freespace] (written with the brackets) was part of the National Day of Civic Hacking, created by the Obama White House, encouraging everyday citizens to get involved in addressing civic issues in their neighborhood. Lipsett, with her team, came up with an idea: “What if we create a community space as a platform instead of focusing on one specific issue?” So, they found a 14,000-square-foot warehouse on the market for $25,000 a month and convinced the landlord to rent it to them for $1. This was the birth of [freespace]. The project had two rules: everything had to be free, and everything had to be participatory.
“It opened up as an experiment, we didn’t have goals or expectations, we didn’t know where it would go,” Lipsett recalls. But the success was hard to believe. “People would come for one thing and stay for another.” There were paella cooking lessons while artists were making sculptures during a class for programming LED Lights. At one workshop, facilitators encouraged kids from the local Boys and Girls Club to create their own superheroes. Then, costume designers turned their visions into reality, working with the kids to create personalized superhero costumes. This likely would not have happened if not for the random human collision which [freespace] cultivated; the workshop idea came to the costume designers after spending time in [freespace], often surrounded by children. Seeing the benefits of giving the community a space with an open invitation to do and create anything inspired a whole [freespace] movement: While the space in San Francisco was always meant to be temporary, 26 different locations opened across 18 countries around the world.
This year, Lipsett mentored yet another Big Ideas team. She values investing time to enhance and encourage students’ social innovations. And while she has decades of experience and serves as a mentor, Lipsett still feels she has a lot to learn from others, whether it’s kids with superhero dreams or grad students providing safer alternatives to police calls. “Working with such determined students is so energizing, the whole process is definitely mutually beneficial,” she says.
Cleveland Justis, professor of MDevEng’s “Introduction to Social Entrepreneurship,” fights these misconceptions by teaching how business strategy can be used as an instrument of social change.
When Master of Development Engineering students find out about the core class on social entrepreneurship, some tend to be a little skeptical. Some, having learned to eschew capitalist norms in previous work and academic experiences, now wonder how a class that teaches market-oriented approaches will be beneficial. Cleveland Justis, professor of MDevEng’s “Introduction to Social Entrepreneurship,” fights these misconceptions by teaching how business strategy can be used as an instrument of social change.
Justis started his undergrad at Swarthmore College and then fell in love with UC Berkeley when he spent the summer in Berkeley after his freshman year. The university, the town, and especially the outdoor scenery prompted him to transfer; one year later, he was a Cal student, studying environmental science. Justis found his passion for environmental education working with Cal Adventures promoting outdoor skills and activities. Immediately after graduating, Justis became an instructor at the National Outdoor Leadership School, leading hiking and kayaking expeditions across Alaska, Chile, and Mexico, while also at the Headlands Institute, another environmental educational nonprofit. While dedicating 10 years each at both organizations, Justis discovered an interest in the strategy side of running nonprofits, an intersection he had not heard much about. “Environmental activists always seem to disagree with business,” said Justis. “But I was dedicated to reconciling that.”
Tackling this goal led him back to school to obtain an MBA from UC Davis Graduate School of Management. Coming from a family of entrepreneurs working in poverty alleviation, Justis knew he did not want to use business school to make companies wealthy, but to create social change. While pursuing his MBA, he began operating under a then-new concept: social enterprise. He identified three crucial facets that remain fundamental to his curriculum to this day: using the tools of nonprofits, government, and business in creative ways to bolster social change. He wanted to understand business as a way to uplift other fields.
Justis wasn’t alone in his curiosity about social enterprise — other students were hungry for it, too. Upon completing his MBA, the dean of the School of Management encouraged Justis to start the first-ever social enterprise course at the business school. So he did just that, formulating a class from scratch. He pulled in guest speakers, many from the government, with the goal of bridging the business-versus-public sector divide. And he soon realized that he really loved teaching — even more than his day job at the time, leading the Golden Gate National Parks Conservancy, a non-profit that supports park conservation throughout the Bay Area.
Despite some hesitation that it was too late and he was too busy to go back to school, Justis returned for an interdisciplinary Ph.D. at UC Davis, working with top-notch faculty and researchers from the business, geography, and community development schools to create unique ways to apply business techniques to create social change.
While working on his Ph.D., which he finished four years ago, Justis was also teaching social enterprise to undergraduates at UC Berkeley’s Haas School of Business. In early 2020, a professor at Haas’ Center for Social Sector Leadership reached out to him and mentioned the start of a new master’s program housed at the Blum Center for Developing Economies: Developmental Engineering. The MDevEng needed someone who could bridge the different worlds of social change and business planning. And this was Justis’ forte.
Justis has taught DevEng 204: Introduction to Social Enterprise since the program’s start two years ago. MDevEng students are required to take the course in their spring semester, learning how to incorporate entrepreneurial approaches to their personal social ventures. This is especially useful to the degree’s required capstone project. Justis has one main goal in his class: help students understand how successful social change requires government, business, and nonprofits to coexist by pulling in strategies across disciplines. Some students tend to be a bit skeptical of capitalist-oriented approaches. “And this is good, it’s a healthy apprehension,” Justis contends. “But I want to help them understand that government hasn’t been universally beneficial either, and non-profits also don’t always act in the people’s best interest.” The ideal system? One which creatively melds all three approaches.
Courtesy of Cleveland Justis
Justis formats his class with some lecturing in the beginning and a substantial amount of time for students to discuss and learn from each other. “The past two cohorts have been very intelligent and great critical thinkers; it’s really impressive,” says Justis. “And I am continuously amazed by how students use their international knowledge and connections to apply my lessons on a global scale.” Justis also brings in guest speakers throughout the course, many of which are based outside the US and represent marginalized groups across the world. And through learning from these speakers, lectures, and each other, students understand the magnitude that small-scale models, ones they can devise and develop within their own networks, have in forging social impact. For example, Mathews Tisatayane, is working to provide his community in Malawi clean energy, healthy food, and economic independence by using a social enterprise for-profit system. This is exactly what Justis hopes students get out of the class — developing impactful models doable at an individual and community scale.
Students in this year’s DevEng 204 class had a new pedagogical tool: Justis’ recently released book Don’t Lead Alone, a culmination of his work, combining the tools he learned through research and valuable lessons he’s learned through teaching social entrepreneurship and leadership. Don’t Lead Alone’s goal is to make his past work more readable and accessible to everyone beyond academia, and it was inspired by students he has inadvertently learned from in his previous classes. The book — Justis’ first — encourages readers to “think like a system, act like a network, and lead like a movement,” drawing skills from leaders across — guess where — businesses, nonprofits, and governments. Daniel Student, a fellow UC Davis MBA alumnus and theater director and actor, co-authored the book and provided creative direction to Justis’ academic linear. Three years of on-and-off writing paid off. Since its release in February, it has landed on at least three different Amazon bestseller lists. But, ever the educator, Justis is most interested in how the book lands with his pupils. “I wrote the book for my students,” he says, “so they’re the true test-case.”
While the paths taken by the 60 newly minted GPP alumni to and through the minor differed greatly, they ultimately converged May 15 at Sutardja Dai Hall’s Banatao Auditorium following classes on poverty alleviation, a hands-on “practice experience” combining theory with practice, and deep reflection on what they learned. GPP’s 16th graduating class drew from 25 different majors and has joined an alumni community numbering over 1,000.
Thomas Kouyate and Samyukta Shrivatsa (Photo by Amy Sullivan)
Samyukta Shrivatsa arrived at Berkeley knowing the huge privilege it was to receive an education at Cal — indeed, what a huge privilege it was to even afford the flight all the way here from India. She came in wanting to change the world for the better, and do so “with an A-plus.”
Then the pandemic hit. The magnitude of the problems it caused and revealed left Shrivatsa, a peer advisor of the Global Poverty and Practice minor who graduated last week, feeling ready to throw in the changemaker towel.
But that was when she discovered the GPP minor — “or perhaps,” she mused to her fellow graduates, “when GPP found me.”
Photo by Amy Sullivan
While the paths taken by the 60 newly minted GPP alumni to and through the minor differed greatly, they ultimately converged May 15 at Sutardja Dai Hall’s Banatao Auditorium following classes on poverty alleviation, a hands-on “practice experience” combining theory with practice, and deep reflection on what they learned. GPP’s 16th graduating class drew from 25 different majors and has joined an alumni community numbering over 1,000.
“We went into this thinking we were alleviating poverty for others,” said Shrivatsa, who is preparing to start an environmental engineering PhD at Stanford, “but we came to understand that we were really doing this for ourselves and that there is infinite hope in recognizing that, thankfully, none of us are alone in shouldering this responsibility.
“There is so much power in recognizing the process of working for change as its own reward: All one has to do is stay the course, regardless of where the path leads.”
Prof. Dan Fletcher, faculty director of the Blum Center, which houses the minor, pointed out that the graduating class weathered pandemic disruptions in the classroom, during their practice experiences, and in their personal lives — not because the GPP program was required of them but “because of their commitment to these ideals.”
“As champions of social justice,” Fletcher said, “they represent the best of UC Berkeley.”
Keynote speaker Prof. Aarti Sethi (Photo by Amy Sullivan)
Keynote speaker and anthropology professor Aarti Sethi marveled at students’ ability to accomplish all that while having to do so much to take care of themselves, their families, and others. “Thank you for teaching us about resilience,” she said.
Sethi asked students to consider the “heart of the liberal university”: libraries — those “spaces of autodidactism” where one could discover the world’s vastness and interestingness, be transported to new places, find intellectual freedom, and wander without purpose. In a world where the uneven distribution of power and resources divides us into those who must “live in need” and those with the privilege to “live in desire,” it’s the latter — a cultivation of “impractical pleasures” — that is a worthy goal to pursue not just for ourselves but for others.
All people have a right to to build an “impractical relationship to the world,” Sethi said. “What an education here can do and should do is to question this division and to create conditions in which everyone can live without purpose in some aspect of their life.”
Thomas Kouyate, a molecular and cell biology major preparing for a position at Boston Children’s Hospital, recalled the minor as one of Berkeley’s biggest draws. He grew up in Senegal and remembers seeing poverty everywhere while he and his friends had the latest material goods. For a time, he accepted that reality.
Understanding the roots of poverty came through interactions with his classmates, faculty, GPP staff, his parents, and “debunking those lies we were taught” about what causes such stark inequality. “We’re not here to solve poverty in a single day,” he discovered, “but rather that we’re here to understand that it starts with us, one day at a time, at a small scale.”
Alumna speaker Peyton Provenzano (Photo by Amy Sullivan)
Kouyate took that wisdom back to Dakar, Senegal, where he did his practice experience at a hospital and with the country’s National Tuberculosis Control Program. He implored his classmates not to become inured to the giant, complicated issues they’ve committed to grappling with: “My hope is that we keep serving and loving those in need, knowing that they will not be able to pay us back.”
That kind of optimism was what alumna speaker Peyton Provenzano most liked about being a student at Berkeley — that students could make their campus and the world a better place.
“The challenge for all of you will be translating that optimism and spirit of the Berkeley campus into your lives beyond the university,” said Provenzano, who just finished her JD at Berkeley Law. “It’s not naive to believe in the prospect of a more just, equitable, and kind world.” The students before her, she added, are uniquely equipped to be the change they want to see.
But progress won’t be linear, Provenzano warned; the inevitable setbacks can’t be cause for discouragement. “Contributions large and small do make a difference.”
For Shrivatsa, these large and small impacts, as well as how the graduating class arrived at them in the first place, form the stories that shape how we see the world around us.
“GPP has been a process of tearing down everything we thought we knew about the world and rewriting the stories we tell about it,” she told her peers and commencement attendees. And the story that GPP tells “is one of audacious hope in the world and each other.”
Following months of designing, workshopping, mentoring and pitching, High Tide, a student team working to produce a bio-based coating for compostability and recyclability, took home top honors at the 2023 Grand Prize Pitch Day and Awards Celebration, the Rudd Family Foundation Big Ideas’ annual finale.
Kira Erickson and Ivan Jayapurna were awarded the Rudd Family Foundation Big Ideas Grand Prize of $10,000.
Following months of designing, workshopping, mentoring and pitching, High Tide, a student team working to produce a bio-based coating for compostability and recyclability, took home top honors at the 2023 Grand Prize Pitch Day and Awards Celebration, the Rudd Family Foundation Big Ideas’ annual finale. Judges gave High Tide, one of 23 finalists to appear at the May 3 event at UC Berkeley’s Blum Hall, the $10,000 Grand Prize.
High Tide, led by Ivan Jayapurna, a PhD candidate in Applied Science & Technology focusing on biodegradable plastics and Kira Erickson, MBA candidate, is dedicated to ending the use of plastic-coated paper in single-use containers unable to be composted or recycled. Their solution prioritizes structure over chemicals, using renewable resources to create a water repellent bio-based coating that will harmlessly degrade in natural ecosystems and can safely fall into green and blue waste bins.
“The past few months have been hectic but fun and definitely educational. We got to talk to a lot of experts and I personally learned a lot about the packaging industry and on developing new materials from a commercial perspective. Today was really cool to see it all come together, as well as seeing all the other really cool projects,” said Jayapurna. “Hopefully this big idea can be a small part in helping us achieve a waste free future.”
“The concept behind High Tide was born out of a realization that the majority of our paper products are destined for landfill, despite paper being a compostable and recyclable material,” added Erickson. “It’s an extremely pervasive, yet less widely known issue. The potential for systemic impact is massive if addressed properly. I hope it’s a challenge High Tide can help solve with our nature-inspired solution.”
This year, the Rudd Family Foundation Big Ideas received 160 applications from UC Berkeley students and 30 applications from its partner campus in the UK, the University of Sussex — representing more than 600 students, 60 disciplines, and 15 countries — all aimed at addressing pressing social issues from food insecurity to workforce development to maternal healthcare. Of the final-round teams, over half of the projects were led by women. During the pre-proposal application period, Big Ideas provided students with a wide variety of resources including entrepreneurship skills workshops, team-building development, networking opportunities, and startup advising. Twenty-three finalists emerged from the 190 applications after a review by over 150 experts from academia, industry, and the venture community. These 23 teams continued to receive support and even more personalized mentorship as they prepared a final application. In addition to participating in today’s poster session, 5 of the 23 finalists were also chosen to pitch their innovations to three judges.
Big Ideas honored Jill Finlayson and Steven Horowitz for their long-time commitment to UC Berkeley students as Big Ideas’ mentors and judges. This year marked Horowitz’s 10 year mark with Big Ideas. Finlayson has been with the program for more than 12 years.
“These finalists are the best of the best of social innovation,” saidJill Finlayson, Managing Director of the CITRIS Innovation Hub and a Big Ideas judge for the last decade. “They could all easily go out in industry and make the next step. But Big Ideas is about making that big leap, pushing boundaries into reality. And that’s where we felt the winning team stood out.”
“It was such a thrill to bring the idea to life with Ivan and with support from our mentors, Tony [Kingsbury], Mathieu [Aguesse], Karenna [Rehorn], and Phillip [Denny],” Erickson said. “We got to meet and learn from many more people along the way as well who inspired us with their dedication to sustainability and generosity with their time.”
Rick Lyons honors two teams of undergraduate students with the Berkeley Changemaker award
The other headliner of the night was 2ndWind, winner of the Lab for Inclusive FinTech (LIFT) “FinTech for Social Good” Initiative, a parallel Big Ideas track focused on advancing innovations that can unlock the potential of digital financial technologies to benefit underserved populations around the world. The FinTech for Social Good contest is made possible by Binance CharityandRipple Impact. 2ndWind aims to help small and medium businesses continue even when the owners retire. The project creates an efficient platform to facilitate small and medium businesses in this time of transition, allowing owners to achieve their retirement’s goals, while preventing the layoffs often associated with small business closures.
Another highlight of the evening was when two undergraduate teams were recognized by Rich Lyons, Vice Chancellor of Innovation and Entrepreneurship. Blackprint Technologies and the Potion Project each won the Berkeley Changemaker award.
This Fall of 2023, Big Ideas is launching a new effort devoted specifically to climate change challenges in California. It will employ the time-tested Big Ideas@Berkeley Methodology to provide training and seed awards to very early-stage, student-led projects focused on climate change innovations in California.
Big Ideas@Berkeley identifies and encourages students to develop solutions to the problems that matter most to them and their generation. In a year-long process of advising, skills training, mentorship, and seed funding, Big Ideas helps students translate their academic work and their diverse experiences into direct impact.
To date, over 11,000 students from 100 different majors have participated. Of the 550 social impact ventures launched through Big Ideas since 2006, nearly 50 percent are still in operation. With the training and the $3 million in seed funding that the program has invested in these students, they’ve gone on to secure more than $1 billion in additional investment, transforming their ideas into solutions that are now making an impact across the world.
This Fall of 2023, Big Ideas is launching a new effort devoted specifically to climate change challenges in California. It will employ the time-tested Big Ideas@Berkeley Methodology to provide training and seed awards to very early-stage, student-led projects focused on climate change innovations in California.
We encourage you to consider a gift to support Big Ideas@Berkeley students with a donation to the program’s Tackling California Climate Change effort — part of UC Berkeley’s weeklong campaign, kicked off during Earth Week, to “spotlight environment-focused projects on campus that are working to create a world where people and nature can prosper.” The campaign ends April 26 at 11:59 p.m.
Learn more about the finalists and their upcoming presentations at the May 3 Grand Prize Pitch Day and Awards Celebration here.
Last summer, Louisa Keeler was in her home state of Texas researching ways the government could support survivors of intimate partner violence. Navigating available resources was difficult, “but trying to get those services while going to school, or raising children, or getting to work — that was much more difficult,” Keeler says. Two colleagues, Ruth Ferguson and Sohail Kamdar, also noticed related themes working with survivors of sexual harassment and discrimination, but also ways in which technology could empower individuals to access secure community services.
Keeler, Ferguson, and Kamdar are all Master of Public Policy students who developed the idea of Sepal, “a simplified, safe haven for finding the care you need by thoughtfully connecting you to knowledgeable providers.” Their idea secured them one of the 19 final-round spots in the 2022–23 Big Ideas Contest, UC Berkeley’s flagship social innovation program. This year, the contest received 160 applications from UC Berkeley students and alumni — representing more than 500 students, 80 disciplines, and 15 countries — and addressing pressing social issues in everything from food insecurity to workforce development to social injustice. Of the final-round teams, half of the projects are led by women and half have a URM co-founder.
Learn more about the finalists and their upcoming presentations at the May 3 Grand Prize Pitch Day and Awards Celebration here.
Farhiya Ali joined Blackbook University as a development intern in 2019 after Ibrahim Baldé, one of digital platform’s founders, reached out to the Black campus community seeking women in STEM to be a part of the organization, which equips Black students with relevant information, opportunities, and a network to connect with their peers.
Farhiya Ali joined Blackbook University as a development intern in 2019 after Ibrahim Baldé, one of digital platform’s founders, reached out to the Black campus community seeking women in STEM to be a part of the organization, which equips Black students with relevant information, opportunities, and a network to connect with their peers. Ali’s passion for accessibility and using technology for social good drew her in. Through her involvement with the 2020-21 Big Ideas winner, the first-generation college student and child of Somali immigrants bolstered her service to — and helped bring together — the Black community while developing her technological skills.
Ali, a senior born and raised in the Bay Area, describes Blackbook University as “a diversity, equity, and inclusion solution to empower Black students and enable peer-to-peer connection, academic enrichment, and professional development.” Currently, the platform connects students with on-campus organizations and alumni through its mobile application. Blackbook hopes to create connections between Black students on campus while utilizing its alumni network to create opportunities for current Cal students.
During her internship, Ali analyzed the enrollment trends of Black students going back to the 1990s, helped create the initial mobile application, and directed social media content. While working on the application, she tested prototypes, worked on the user interface, and conducted user interviews about how to improve the mobile app. She learned how to connect each page of the mobile application so they were easily accessible.
Ali says Baldé consistently encouraged her and the rest of the Blackbook team to take ownership of their work. “You had his full support to explore different areas of the company and take ownership,” she recalls. “Or, if you saw that someone was working with some really cool data sets that you want to work with, you have full support to go work on that and explore that area.”
During her sophomore and junior years, Ali moved up to a product marketing role within Blackbook and is currently its user design/experience expert, where she continues working on the mobile Blackbook University application, available for download on the App Store and Google Play Store.
“We want [the app] to be a space where alumni can reach out and provide students with opportunities,” Ali says. (The team is currently building toward securing angel funding.)
In addition to benefiting her peers, Ali’s tenure at Blackbook has developed her own professional repertoire in, among other things, software development, product management, and creating social campaigns — and all while exploring different disciplines through her projects and team members, whose majors range from data science to legal studies, business administration to media studies. She’s utilized platforms like Excel, Asana, and Trello, though some of the most important skills she says she learned were interpersonal skills, like “how to communicate differences professionally and how to maintain a level of respect, accountability, and transparency within a team.”
All of these skills and experiences came in handy during her fast-paced internship last summer at Kinestry, an innovation studio that helps clients develop meaningful brand experiences through technology and specializes in non-fungible tokens (NFTs). One of her projects at Kinstry was Metaverse Fashion Week, a completely virtual fashion week that allows designers to showcase their work digitally. Thanks to her Blackbook experience, she was able, in her collaboration with clients, to make sure artists felt their projects were feasible and their work valued. Her experience with user interfaces and interviews at Blackbook helped her as a Kinestry product manager to gain insight into how to best assist clients in meeting their goals as well as staying organized in her own work.
Ali, however, has actively supported Berkeley’s Black student community beyond Blackbook. She’s been involved with the Black Engineering and Science Student Association since her sophomore year, when she started as BESSA’s pre-collegiate outreach chair. Founded in 1968, BESSA’s mission is “to increase the number of culturally responsible Black engineers and scientists who excel academically, succeed professionally, and positively impact the community.” Now, as president, Ali leads a team of 12 other board members whose programming focuses on K-12 outreach in the Bay Area, study jams, tutoring, and corporate-sponsored events for current UC Berkeley students. As president, she launched a paid, peer-to-peer tutoring program for Black STEM students as a form of academic retention and supports fundraising to sponsor students’ trips to national conferences.
Ali also credited a change in major to opening up opportunities to serve her peers. She started out in electrical engineering and computer science (EECS), but that changed in spring 2022 when she took a gap semester to take community college classes and network to expand her professional opportunities. During the break from Cal, she spoke with friends and people in her network and learned more about the Interdisciplinary Studies Field major, “what it did for them, and what doors it opened.” These conversations inspired her to switch from EECS to ISF, with a focus on human-computer interaction, in order to further serve the Black community on campus and pursue internship opportunities — the latest being a technical project management internship at Dolby Laboratories. The lighter load of the ISF major allowed her to both earn a fulfilling degree while having enough time to devote herself to other opportunities outside of academics and serve her community.
Throughout her time in university, Ali has had mentorship from other students and alumni, from Baldé to her BESSA predecessors. Now an upperclassman herself, she’s taken up the role of giving back to underclassmen. “You should move forward,” she says, “but always give back to the community that helped you get where you are.”
Tisatayane had been a teacher, a nurse, and an unsuccessful social entrepreneur. Now, he’s using development engineering to provide his fellow Malawians clean energy and an opportunity to free themselves from economic hardship.
Tisatayane had been a teacher, a nurse, and an unsuccessful social entrepreneur. Now, he’s using development engineering to provide his fellow Malawians clean energy and an opportunity to free themselves from economic hardship.
Growing up, Mathews Tisatayane had few boundaries about where he could go and who he could see. His corner of Malawi, in southeast Africa, was multicultural, and he hung out with people from different tribes, who spoke different languages, and who practiced different religions. He didn’t have electricity or running water, and his family took him shopping for clothes once a year if he was lucky. But “growing up,” he said, “I didn’t feel like I was poor at all.”
As the third child and first-born son of his mother’s 12 children, he held a lot of responsibility and worked on his family’s farm growing tobacco — a major component of the Malawian economy. When he was seven, he used the income he earned to self-enroll in a school about five miles away.
Mathews Sapemba Tisatayane (Courtesy photo)
Tisatayane, now 50 and finishing his final semester of UC Berkeley’s Master of Development Engineering program, says his family still grows tobacco “out of desperation, out of ‘what else can we do?’”
When he finally did get the chance to go to school, he encountered his first Peace Corps volunteer, which made him think the U.S. had something to offer the world. These ideas lodged in the back of his mind.
Tisatayane finished high school in 1994, but the introduction of college-entrance exams that favored elite kids halted his plans for college. It was already a dark time: His great uncle, who owned his family’s farm and had funded everything in his life, had passed away. He recalled trying to compose himself and asking what he could do in this bleak situation.
If there is one thing that defines Tisatayane, it’s resilience: “When I’m put in a situation, no matter how bad or good it is, I’m always trying to say, ‘How can I do better for myself and the people around me?’”
The mantra has guided him through famine, nursing school, full-time nursing, a deep but unsuccessful foray into social entrepreneurship, all the way to the inaugural cohort of the M.DevEng program. During his three semesters at Blum Hall, he parlayed new professional and peer connections to launch Umodzi with Sean Mandell, a recent graduate of the Haas School of Business at UC Berkeley. The company is a reincarnation of Tisatayane’s failed attempt at social entrepreneurship, allowing women-led co-ops in Malawi to raise quail in a 100-percent sustainable, self-contained system.
“I’m almost happy I failed,” he said of his first attempt at sustainable development. “If I didn’t fail, I wouldn’t have come to Berkeley.”
From famine to the San Francisco Department of Public Health
After his great uncle died, Tisatayane found his way to a teacher’s training college, spent two years there, and returned to his village to teach kids — all while continuing as a subsistence farmer providing for 17 people as the elder man of the family.
But more hardship was in store. In 2001, a terrible famine hit Malawi. Tisatayane lost half his body weight and, at one point, while still teaching, went three days without food. The problem, he realized, wasn’t that there was not enough food in the country, but that it was not accessible to poorer people — including those who grew it. “That was the famine that changed my life for good,” he recalled two decades later. “It’s one of the things that pushed me to” apply to UC Berkeley — “to try to do something to relieve my people of that.”
Meanwhile, he had gotten involved in a government program where people planted trees for food. There, he met another Peace Corp volunteer. They married. And that was how Tisatayane made it to the country that, in high school, he started to realize had something to offer the world.
“When I came to the United States, I was totally useless,” he said. In Malawi, he had friends, family, a teaching job. “I had everything there. And then all of a sudden, I’m in a completely different situation.” He was lost. It was like the end of high school all over again.
But that spurred the same thought process: What could he do to help himself and those around him? Tisatayane enrolled in the City College of San Francisco not knowing what he wanted to pursue. But it reminded him of his youth, surrounded by folks speaking different languages, practicing different religions, displaying different personalities. It buoyed him.
While at CCSF, Tisatayane volunteered for six months in the unit serving patients with HIV/AIDS, learning about U.S. patient care. Many of them nearing the end of their lives didn’t have family, and he saw how the nurses became the closest relationships they had. “The passion, the love, and the dedication of the nurses who worked in that care unit,” he said, “inspired me to be like, ‘I think I want to be a nurse and do what these people are doing.’”
He studied intensely and improved his grades while at CCSF but did not get into the nursing program there, which used a lottery system. Persevering, Tisatayane later found a different school, and he became one of the very few men or Black people in the University of San Francisco’s undergrad nursing program, from which he graduated with a bachelor of science in nursing in 2011.
With the mission of helping the homeless suffering in the wealthiest country in the world, over the next five years, he worked at the San Francisco Department of Public Health’s Medical Respite & Sobering Center, aiding those who were discharged from the hospital and needing housing or social services as well as those passed out on the street and smelling of alcohol. Despite the 11 p.m. to 8 a.m. shift — and the beginning of a new family here — Tisatayane continued to support his family back home in Malawi.
“If you’re not going to do this, you’re going to regret it on your deathbed.”
Though he had spent years helping those in need in San Francisco, his family in Malawi continued to grow and need support. His sisters and their friends had started a cooperative, Yankho co-op in Kauma Village, and he gave them $5,000 to use however they wanted. Six months later, the group of women had started an informal microfinancing program among themselves; every Sunday, they got together to lend money to whoever needed it most that week.
Tisatayane found that many women, along with their children, were raising chickens and other small birds, but they couldn’t scale their efforts. The cause mirrored that of the famine: Bird-feed ingredients grown in the village were bought up by middlemen, who sold them to businessmen in the city to make the feed, and who then sold it back to the farmers. He wrote up a business plan and showed it to contacts of his wife, who secured him $35,000 in funding. He would bring to his community a self-sustaining bird-raising operation.
The key, he learned, was energy: ubiquitous in the U.S., scarce in his hometown. He studied microgrids — small-scale, self-sufficient energy systems — and reached out to friend and fellow Malawian William Kamkwamba, of The Boy Who Harnessed the Wind fame, who put him in touch with someone who got him the solar panels and batteries that Tisatayane would assemble into bird incubators and brooders. The equipment was paid for using the funds Tisatayane had raised.
The incubators could replace a hen lying on her eggs for 21 days — not an easy model to scale — in order to hatch as many eggs as possible. The chicks would then stay in the brooders — warm rooms that mimic their mothers’ feathers. After two weeks, the birds would be ready to be sent to farmers.
Solar panels being installed during Tisatayane’s first attempt at sustainable development in Malawi. (Umodzi photo)
If his community could raise their own chickens all on their own, then they would eat well, which meant better health. They could sell the ones they couldn’t eat for income. And building a system run by women and youth would empower them, too. One of “the most profound moments” in the process, he recalled, was being in the U.S. and receiving a video of incubated chicks hatching at his village — “life coming out of an egg, because of the invention that we made.”
The machines worked well for two months. When they started failing at night, he hired independent solar companies to check them out. The panels, it turned out, had come from different manufacturers, as did the wiring. Either they were put together improperly or the batteries were used too quickly and died. The endeavor was paused indefinitely.
Tisatayane said he felt like “a failed social entrepreneur.” He tried out some online courses on social entrepreneurship, but they didn’t help. Then, he discovered UC Berkeley’s Renewable and Appropriate Energy Lab, run by Prof. Daniel Kammen. He spent a week on YouTube devouring Kammen’s talks. He wanted more. “How can I be part of people like this,” he asked himself, “because I truly, truly believe that I can do more in Malawi.”
In following the lab online, he came across Berkeley’s new Master of Development Engineering program, the first cohort of which was to start in the fall of 2021. “This is it,” he thought. “If you’re not going to do this, you’re going to regret it on your deathbed.”
Investors and biodigesters
Sure enough, he was accepted. He’d wake up at 6 a.m., take BART from his home in southern San Francisco to downtown Berkeley, and hike a mile up through campus to California Memorial Stadium for DevEng C200, “Design, Evaluate, and Scale Development Technologies,” at 8 a.m. He had started his dream program, a chapter in his life he hadn’t even considered not long before.
Sean Mandell (Courtesy photo)
That first-semester M.DevEng course turned out to be pivotal. Tisatayane met Sean Mandell, a student at the Haas School of Business who had been a data scientist for four years at a health-tech start-up. Mandell had had a longtime interest in — but limited involvement with — global development and had come to Berkeley to pursue social entrepreneurship. The two chatted during class breaks.
“We truly liked each other and respected each other’s views on what needs to happen in terms of development,” said Mandell, who graduated in May.
“Without Sean, my business wouldn’t be what it is,” Tisatayane said on a recent afternoon at a cafe on Euclid Avenue, near Blum Hall, home of the M.DevEng program. He described their blueprint: Solar panels heating multiple hatcheries incubating quail eggs, and biodigesters turning quails’ waste into fertilizer for the birds’ food as well as fuel to supplement the solar electricity. Once up and running, the circular system could address a panoply of the United Nations’ Sustainable Development Goals, including zero hunger, gender equality, affordable and clean energy, responsible consumption and production, and more. The whole enterprise, which they named Umodzi — “togetherness” in Chichewa, one of Malawi’s main languages — would be run by the women cooperative with whom Tisatayane had collaborated on his first try. The name reflected the unity with which Tisatayne’s community approached everything, from work to celebrations, as he grew up.
A biodigester at Kauma Village (Photo by Sean Mandell)
Prof. Layla Kwong of the School of Public Health, his capstone advisor, gave him the idea to use biodigesters — mechanical stomachs that convert organic material, like quail poop, into biogas to heat incubating eggs, cook food, or make fertilizer to grow the quails’ food. Tisatayane read up on the process and discovered a biodigester maker already in Malawi. The country also had an incubator maker. “Talking to people, we found out all the systems were already there,” he said.
Eventually, Tisatayane and Mandell registered Umodzi as a public-benefit corporation in the U.S., with a subsidiary company in Malawi and a lawyer in each country, too. Tisatayane is founder and president; Mandell, co-founder and CEO. They went on to raise over $100,000 from individuals interested in supporting their project and even contributed some of their own savings. They bought a 25-kilowatt solar power system with a 60 kilowatt-hour lithium battery system from a Malawian supplier.
But getting a fully functioning enterprise off the ground required even more investment, and that’s where networking through the M.DevEng program came in handy once again. Prof. Alice Agogino, chair of the Graduate Group in Development Engineering, introduced Tisatayane to Stephen Isaacs, former president and CEO of Aduro Biotech and a member of the program’s advisory board, who then introduced him to his own friend Bob Reed, former CFO at Sutter Health. Reed immediately took to the idea. “What can I do for you?” he asked Tisatayane.
“I have an idea to change my community, but I know nothing about the money world,” he had replied.
Reed enthusiastically obliged and became a friend and mentor to Tisatayane, introducing him to another potential investor. Umodzi’s circle of backers grew.
“Here for the indefinite future”
In the spring, Mandell surprised Tisatayane: He had bought a one-way ticket to Malawi, departing the day after his May graduation. “I’m here for the indefinite future,” Mandell told him.
Tisatayane himself left for the country in June and stayed for two months, his longest trip to Malawi since moving to the U.S. Gut instinct told him to stay for a second month; it allowed him to be with family when his father passed away.
Solar batteries and an inverter (Sean Mandell photo)
The batteries (lifespan: 10-plus years) and electrical equipment arrived in modular shipping containers and joined the hatcheries and biodigesters in Kauma Village. Solar panels (lifespan: 30 years) were installed, and a borehole was drilled to provide potable water to the birds. While drilling, they decided to install taps for the local community to access the water for free.
Umodzi’s fundraising efforts have netted just enough money to launch; Tisatayane estimated all the investment will be recouped in about a year of operations. As site manager, the pair hired Bernadetta Ndongera, a young woman from the community with experience working with farmers, raising poultry, and growing crops and with a degree in agriculture from Lilongwe University of Agriculture and Natural Resources, in the country’s capital. “We didn’t want to bring in a man when both co-founders are men,” Tisatayane said. The Yankho co-op remains Umodzi’s backbone. In fact, it was the women’s cooperative that aspired to raise quail as a ticket to economic freedom and self-sufficiency in the first place.
As his final semester in the M.DevEng program wound down, Tisatayane bought a one-way ticket to Malawi to be full-time hands-on. Before departing in mid-January, he’ll wrap up his current job as a health nurse at a San Francisco County jail, which he had been juggling alongside his studies, entrepreneurial activities, and parenthood. He expects to split his time between the two countries he calls home, with plans to come back to California later in 2023.
With only a couple weeks left in the M.DevEng program, Tisatayane was sent a familiar type of video — the first sign that months of hard work, perseverance, and passion were beginning to bear fruit for his community. Umodzi hatched the first quail chicks from an initial batch of 900 — a mere fifth of the number all its incubators will hold. On his screen, he watched in awe as a few of them broke through their shells.
“My goal is to relieve Malawi of its tobacco industry and replace it with clean energy, and from there, move on to the rest of Africa or the rest of the world, to the extent that we can,” Tisatayane said. “But I can’t clean up Zambia and other neighboring countries until I clean up Malawi, my backyard.”
After 16 months, three semesters, 44 internships, 26 capstone projects, and countless hours in the classroom and out in the field, the inaugural cohort of UC Berkeley’s M.DevEng program walked across the stage of campus’ Sibley Auditorium in the Bechtel Engineering Center on Saturday to receive the country’s — if not the world’s — first master of development engineering degree. The 44-student Class of 2022 — pioneers of the burgeoning discipline that originated at Berkeley — will leave Blum Hall for careers in social impact, technology, and sustainability or to further their educational careers.
The inaugural cohort of the M.DevEng program are the first students — possibly in the world — to receive a graduate degree in the field. (Photo by Amy Sullivan)
After 16 months, three semesters, 44 internships, 26 capstone projects, and countless hours in the classroom and out in the field, the inaugural cohort of UC Berkeley’s M.DevEng program walked across the stage of campus’ Sibley Auditorium in the Bechtel Engineering Center on Saturday to receive the country’s — if not the world’s — first master of development engineering degree. The 44-student Class of 2022 — pioneers of the burgeoning discipline that originated at Berkeley — will leave Blum Hall for careers in social impact, technology, and sustainability or to further their educational careers.
Students and their families, many of whom flew in from around the world, gathered at dusk for an intimate ceremony and reception to celebrate a group hailing from 15 countries and with backgrounds as diverse as education, electrical engineering, finance, and nursing. During their three semesters, the graduates studied a multidisciplinary curriculum focused on design and management of technology, application of emerging technologies, evidence-based assessment techniques, economic development, social problem solving, cross-cultural collaboration, and community engagement. From their first class, they’ve been devising and implementing technological solutions to complex societal challenges in low-resource settings.
Student speaker Mathews Tisatayane (Photo by Amy Sullivan)
“Regardless of the path each one of us is taking, we all agree the world would be a better place if we all put our efforts together,” said student speaker Mathews Sapemba Tisatayane, who took the stage to raucous cheers from his peers.
He began by asking the room to take a deep, collective breath. That breath, he pointed out, is an interaction of, and made possible by, all sorts of elements, from air molecules to lung cells, tissues to organs. “Although all these cells are different in some ways, by working altogether they maintain life as we know it,” he reminded us.
If togetherness is so vital to making the world work, why, he asked, is modern society so resistant to working together to solve climate change and poverty? We’ve been taught to work as individuals and to think of our divisions as almost natural, he said. “But it’s not. I came to UC Berkeley to find minds who could help me challenge these divisions. And I’m happy to tell you I found them,” he said, gesturing to his erstwhile classmates in the front rows. “They’re right here. Through different interactions with each other, faculty, and capstone projects, we researched and found our differences are what bring us closer.”
Tisatayane turned to Nelson Mandela for how the cohort could turn its togetherness into action: “‘Overcoming poverty is not a task of charity. It is an act of justice,’” he quoted. “‘Like slavery and apartheid, poverty is not natural. It is manmade. And it can be overcome and eradicated by the actions of human beings. … Sometimes it falls on a generation to be great. And you can be that generation.’”
“Let us be great. Let us be that generation that Nelson Mandela was talking about,” Tisatayane added. “Let our greatness blossom together. Let’s go out in the world to do actions to positively impact the planet and the lives of those living in poverty. In togetherness, we believe.”
From left: Malika Sugathapala, Daniel Huang, Curtis Wong, and Eleanor Chin (Photo by Sam Goldman)
Tisatayane cited his own capstone project as a product of togetherness. It was a reincarnation of an unsuccessful attempt at sustainable development in Malawi, where he was born and raised. He had teamed up with Sean Mandell, a Haas School of Business student he had met in his first DevEng class, to found Umodzi — “togetherness” in Tisatayane’s native language, Chichewa — which allows women-led co-ops in Malawi to raise quail in a 100-percent sustainable, self-contained system. His classmates’ capstone projects included a business for seamstresses in rural Ghana to sell their high-quality wares, a toilet that recycles the nitrogen from urine to use in fertilizer, advancing an initiative to bring arsenic-safe drinking water to rural cities in California, and a blockchain-certified recruiting platform enabling Nigerian students to close the gap between job seekers and employers.
“What you’ve done with your projects is remarkable,” said DevEng and Energy and Resources Group Prof. Dan Kammen in a recorded message to graduates. “You’ve launched this program with your passion and all the projects you’ve done.”
Commencement speaker Prof. Maya Carrasquillo (Photo by Amy Sullivan)
Civil and Environmental Engineering Prof. Maya Carrasquillo, the newest member of the Graduate Group in Development Engineering, which offers the M.DevEng, gave the commencement address.
“When I learned that this was the first cohort — the first cohort — for the Master of Development Engineering, I felt myself awestricken,” she said.
“You have become the precedent for what this program can and will become: a program marked by educating and equipping changemakers to develop innovative global solutions. What a powerful vision, and each of you embodies that so much,” Carrasquillo said. “It takes a certain kind of individual to step out into unproven, untested grounds. … You’re the ones who dare to do something different, in pursuit of something greater than yourselves. You are the ones not motivated by titles or prestige but by an inner voice that reminds you there has to be more than the way things have always been.”
Carrasquillo offered reflections shared at a book-tour event she attended for former First Lady Michelle Obama’s The Light We Carry: “To treat yourself and others with gladness.”
“In a world and in a profession where we are constantly striving to do good, it is all too easy to forget to be good,” she said. “And more than just being good — being kind — and even then, it is far too often that we are kind to others and less kind to ourselves. As you all go out to do all the amazing, undoubtedly life-changing things that you have been prepared to do in this world, never forget to greet yourself and others with gladness.”
Shubham Salunkhe (left) and Sara Almusafri with Prof. Alice Agogino (Photo by Amy Sullivan)
Early in the ceremony, the M.DevEng program honored retiring Prof. Alice Agogino for her years of service in developing and guiding Berkeley’s DevEng programs, in which she chairs the Graduate Group in Development Engineering, serves as the Blum Center for Developing Economies’ education director, leads the M.DevEng’s Sustainable Design Innovations concentration, led DevEng seminars, mentored many students, and held innumerable office hours with both enrolled students and prospective ones. Director of DevEng Programs Yael Perez presented Agogino with a scrapbook of photos and messages from the DevEng community, and Kammen highlighted her career of developing opportunities for students, faculty, and others to collaborate across disciplines and focus their STEM work on social impact. “What an honor and pleasure to work with you,” he said.
Bioengineering professor and Blum Center faculty director Dan Fletcher closed out the ceremony by noting how clearly the commencement showcased the tight-knit and supportive community the graduates had formed over their three semesters. Each grad walked across the stage to not just a reading of a self-written, third-person statement detailing their accomplishments, but to the cheers of their fellows.
Though classes are over, Fletcher said, “the connections among you continue.” He called out how fitting it was to conclude the students’ recognition with the ending of the final student’s statement: “And she loves you all very much.”
Blackbook University is a digital platform that equips Black students with relevant information, opportunities, and a network to connect with their peers. It was launched to meet the needs of Black students on UC Berkeley’s campus — and to be a model that can be replicated across California, and eventually the nation.
In 2018, the USC Race and Equity Center released a report that measured postsecondary access and student success for Black undergraduates at public colleges and universities across the United States. In this report, the University of California, Berkeley received a C in representation equity and a D when it came to completion equity. According to the report, Black students at UC Berkeley are graduating at a rate of 75.4 percent — 15.9 percent less than the overall graduation rate.
Ibrahim Baldé is a Bay Area native and UC Berkeley alumnus who graduated from the Haas School of Business with a BS in Social Entrepreneurship and Finance in December 2020. The Report led Baldé and a team of peers to question the implications of UC Berkeley’s ranking for Black students and how “community organizers and groups [could] use this to challenge or call out the narrative of UC Berkeley.” Baldé believes that the prestige surrounding UC Berkeley tends to downplay and often erase recognition of the barriers and challenges that underrepresented communities face. He wanted to do something. Blackbook University was the answer.
Blackbook University is a digital platform that equips Black students with relevant information, opportunities, and a network to connect with their peers. It was launched to meet the needs of Black students on UC Berkeley’s campus — and to be a model that can be replicated across California, and eventually the nation.
In its research, the team discovered the legacy of the African American Student Handbook, which served as a resource guide for Black Students at UC Berkeley in the 1980s and 1990s. This resource guide, dubbed Blackbook, listed Black faculty, advisors, student organizations, alumni, and Black-owned businesses that would support students during their time at UC Berkeley. It was a tool “for the community to streamline networking and belonging the moment that someone [touched] base on this campus,” Baldé says.
In 1996, Proposition 209 was passed in California, elimating “state and local government affirmative action programs…based on race, sex, color, or national origin.” Once this proposition went into effect, it significantly decreased the number of Black students admitted to Berkeley, as the University of California system could no longer provide outreach, counseling, and tutoring services targeted at individuals based on sex, race, or ethnicity. Baldé notes that the impact of Proposition 209 on UC Berkeley’s campus was that the infrastructure of the Black community started to diminish and “the resource guide was no longer maintained.”
The Blackbook team came together in 2019 to discuss the importance of the resource guide for students in the past and how they could modernize it to meet the needs of current Cal students. The team included UC Berkeley students Chase Ali-Watkins ’20, Nahom Solomon ’21, Farhiya Ali ’23, Nicholas Brathwaite ’20, and Imran Sekalala ’22. Kyle Parkman, a 2020 UC Santa Cruz graduate, rounded out the founding team.
To assess need, the team polled Black students on campus and found that around 90 percent of Black Cal students wanted a platform for Black students built by Black students. Blackbook was founded on three pillars: an accessible mobile application for students, university programming to empower the professional development of students, and storytelling to highlight the success of Black students and professionals. Blackbook University’s mobile platform connects students to events, opportunities, and programs led by on campus organizations. The team is currently in the process of reaching out to Black student leaders on UC Berkeley’s campus to get them onboarded and to begin utilizing the platform to communicate with Black students.
“We’ve made it so that any Black student can enter the platform and understand exactly what resource or experience is available and optimal for them,” Baldé says.
Currently, the mobile application is available on the App Store and the Google Play Store for download. Blackbook’s goal is to have 500 active users on the platform by the end of the 2022–23 school year.
Blackbook University founder Ibrahim Baldé at the 2021 Big Ideas Grand Prize Pitch Day. (Blum Center photo)
The 2020–21 Big Ideas Contest gave the Blackbook University team the ability to take Blackbook from an idea to a tangible product. The competition helped the team challenge themselves, offered them access to advisors, and helped them structure the model of Blackbook. One of their advisors was Bill Allison, the current campus technology officer at UC Berkeley. Baldé notes that Allison offered insight on how to “think about and navigate both the development of the platform and the onboarding process for our users in our pilot [and] also at scale.” Big Ideas also allowed them to network with several other entrepreneurs who have built other university-based platforms. The networking opportunities showed the Blackbook team it was on the right track, Baldé says. He also credits Big Ideas workshops and advising sessions with helping Blackbook solidify its approach to building their program.
Since winning Big Ideas, Blackbook has continued evolving through app development, a pilot program, and continued involvement in the Black community at UC Berkeley. In late 2021, it created a pilot in collaboration with African American Student Development on Berkeley’s campus to work on projects to integrate Blackbook further into the Berkeley ecosystem. This pilot program consisted of five interns who worked on thinking about and tailoring solutions related to the complexities of Blackbook. They pitched different ideas about the trajectory of Blackbook and how to further leverage technology to positively impact the experience of Black students. The team continued to connect with the Blackbook interns over the summer to ensure that their input was being integrated into updates to the Blackbook application and marketing strategies.
This past summer, the Blackbook team connected with high school Black Student Unions and community colleges to continue their outreach and upliftment of the Black community across the Bay Area. It hopes increased contact with high school and community college students will allow the platform to create meaningful connections with these students and communities before they arrive at a four-year institution.
“We are working to make the Blackbook platform accessible beyond the UC Berkeley campus,” Baldé says. “Our goal is to build a Blackbook presence on every campus in the US, starting with major campuses and the UC system. We see university recruiting as a huge aspect of the growth of our model moving forward — we intend to position Blackbook as the access point for companies and organizations to hire Black talent.”
Global Poverty & Practice peer advisors use the experience they’ve gained in completing most of the minor to counsel their newer peers. Learn how four of them found and added to the GPP community and pursued tangible social impact in their summer practice experiences.
The Global Poverty and Practice minor was the reason Grace Elam ended up at Berkeley in the first place. The university was “way too close to home” for the San Franciscan, and she felt skeptical that Berkeley’s reputation for real-world change had continued to live up to the 1960s’ Free Speech Movement. After receiving an admissions letter, she snuck over to Cal Day to scope things out. She only remembers attending one event: a GPP alumni panel that “shared their experiences building a schoolhouse in Ghana and working in carceral reform in California.” She knew where she wanted to go for college.
Grace Elam photo
The fourth-year, who’s majoring in rhetoric and minoring in both GPP and public policy, has spent the past two summers working full-time in the legal office of the U.S. Environmental Protection Agency’s Pacific Southwest region, and continues working there part time. Much of her work focuses on the EPA’s engagement with other governments, including those of Navajo Nation, Guam, and California, as well as tracking civil rights compliance of grant recipients, processing the public’s requests for agency records, tracking citizens’ environmental lawsuits, researching the history and cultural practices of Native nations, and looking into the community impacts of polluters.
Through “tricks of timing and my own desire to make the most of GPP’s foundational praxis,” the EPA job became her GPP practice experience, the hands-on component of the minor where students apply in the field what they learn in the classroom.Elam is also one of seven GPP peer advisors who use the experience they’ve gained in completing most of the minor to counsel their newer peers.
“I found that GPP was the most welcoming community I had come across at Cal,” said fellow peer advisor Samyukta Shrivatsa. “From the staff to the faculty and students, I owed so many of my best experiences to the encouragement and warmth extended by them. Finding meaning in one’s college experience can be a lonely journey, and I wanted to pass on the support I received to other similarly lost students!”
“Expanding how I look at the world”
Mahima Sinha’s passion lies in increasing access to healthcare in communities. It drove the fourth-year, pre-medical track public health student to take GPP 115, “Challenges and Hopes,” in the first place. What stuck out to her was how the program could be tailored to students’ personal experiences, combined theoretical frameworks with real-world action, and promoted reflection on learnings and experiences. “I learned to think critically about poverty and inequality in a way that I had never thought of before,” Sinha said.
Mahima Sinha photo
But it was the program’s community that also drew her in. “I loved how supportive everyone was of each other and how inclusive it felt.”
Sinha has stayed close to home with her practice experience, which can take students around the world. She continues to work remotely with Transitions Clinic Network, a San Francisco–based nonprofit providing healthcare services to those transitioning out of incarceration, doing data analysis of patient demographics, designing a manual for the TCN’s healthcare hotline, writing articles for San Quentin Prison’s social justice–oriented news site, and interviewing TCN’s community health workers — folks who have been incarcerated whom TCN hires to “create a supportive healthcare experience for patients and support their autonomy,” Sinha says.
“I have been able to learn so much about the effects of mass incarceration and how that impacts health specifically,” she said. “It has been challenging because I have never worked with the reentry population before and I am learning a lot as I go, such as the proper language to use, the harmful stigmas associated with incarceration, and the increasing need for reentry services in the United States.”
Expanding her perspective has been a key element of her overall GPP experience, which is open to all majors, allowing for a wide array of outlooks and frames of reference.
“This has really expanded how I look at the world and analyze what I see in the news,” Sinha says. “The minor has also offered me a lot of insight into how I can incorporate these frameworks into my future career, regardless of what I end up doing.”
“A lot of ownership for this project”
Also a fourth year, Samhita Bhat studies public health and molecular and cell biology.
Over this past summer, she worked at Public Health Research Institute of India (PHRII), a nonprofit in the southern city of Mysore that researches women’s reproductive health, runs education and screening programs, and offers health services. As her practice experience, Bhat evaluated the impact of PHRII’s cervical cancer screening program through interviews with local community health workers, who were often overburdened managing the health of thousands of rural community members. She brought with her fluency in Kannada and, “as the daughter of immigrants from the state of Karnataka, a lot of personal knowledge and deep-rooted connection to the poverty that community members experience there.”
Her internship work resulted in a research abstract she presented at a conference and will be published soon in Annals of Epidemiology. “I felt a lot of ownership for this project as I was able to conduct interviews on my own,” Bhat said.
What’s helped cement her interest in continuing to work with healthcare-oriented grassroots organizations, she says, has been a curriculum that’s allowed her to better confront her own privilege and recognizing “the harm that my own actions may have in conducting poverty alleviation and how to mitigate that.”
“GPP has been a really special and unique part of my Berkeley experience, and I felt like I found a really strong community within my GPP classes and cohort,” Bhat said. Being a peer advisor, she added, allows her to transmit that experience to others while connecting with peers who have similar interests to hers. “I love hearing about the various passions and experiences that such a diverse group of students have within the minor.”
“Challenging these systems in my professional and personal life”
“I was very aware of the privilege that an education at Cal gives me,” recalled Samyukta Shrivatsa, a senior studying environmental engineering science, “and was interested in understanding the education system I grew up with, the role education has to play in social and economic mobility, and how we can better serve students who go through the system.”
Samyukta Shrivatsa photo
Shrivatsa came to the US from Bangalore. “Navigating college as an autistic student during COVID-19 was very challenging.” But it brought with it an awareness “of the complexities of privilege and power omnipresent in my life” and the desire to find a way to leave the world better off than how she’s found it. GPP 115 convinced her that “engaging in meaningful activities of solidarity” was where she wanted to be.
To these ends, she returned to Bangalore this past summer with Parikrma Humanity Foundation, which provides a holistic education to students from marginalized socioeconomic backgrounds. She had been intrigued by the way the school supported its students emotionally, medically, and financially since meeting some of those students in high school.
“I realized very quickly that my role as a temporary volunteer was miniscule, and that I had to think carefully about what kind of work I could do that would be most helpful to teachers with decades of experience,” she said. Shrivatsa observed the love with which the teachers approached their students’ difficulties. Her own days varied widely: playing football with students one day, talking K-dramas another day, introducing them to parliamentary debate yet another day, and all the while hearing out their backstories, hopes, and dreams.
For Shrivatsa, the practice experience and her classes have been a source not only of extensive knowledge, a realization of how much she doesn’t know, and how to be critical of “the systems and rhetoric surrounding issues of poverty and development,” but has given her the tools to “challenge these systems in my professional and personal life.”
“Celebrating the importance of their work and passion”
“I’ve landed in a front-row seat for US federal environmental governance, which is fascinating to watch, and extremely complex to be a part of,” said Elam of her EPA job. Some of the public’s preconceptions about the federal government, she found, aren’t far off, like dense bureaucracy and “high-level political indifference” slowing the pace of the government’s justice work. But that front-row seat also hit home that the EPA and its sibling agencies are made up of people at every level, who do good work and bad, “occupying different roles and having different impacts, and most importantly, responding to different pressures as ordained by their roles.”
In her second year, in an unrelated campus organization, she got to know a peer advisor, who became a mentor not only in GPP but for her whole Berkeley experience and work in social change. “I missed her when she graduated, and thought of her immediately when last spring I received an email from the GPP minor suggesting I apply to be a peer advisor,” she said. “Partly in her honor, and partly because I was flattered by the anonymous nomination, I did so and applied, and now I’m here!”
During advising sessions, Elam continues to draw inspiration from the peers with “their passion, drive, and ideas for their own GPP trajectories.”
“I believe in those students, and I want to celebrate the importance of their work and passion, and to set them up as well as I can to have their desired impact on the world and their issue of choice,” she added. “I’ve found that I leave every advising appointment I have with a smile.”
Host and Fellow Responsibilities
Host Organizations
Identify staff supervisor to manage I&E Climate Action Fellow
Submit fellowship description and tasks
Engage in the matching process
Mentor and advise students
Communicate with Berkeley program director and give feedback on the program.
Berkeley Program Director
Communicate with host organizations, students, and other university departments to ensure smooth program operations
Student Fellows
Complete application and cohort activities
Communicate with staff and host organizations
Successfully complete assignments from host organization during summer practicum
Summarize and report summer experience activities post-fellowship